The first major branch of the abdominal aorta at T12. Three branches, six board traps, and the watershed zones that kill colons.
A patient with a posterior duodenal ulcer presents with massive upper GI bleeding. Which artery is most likely eroded?
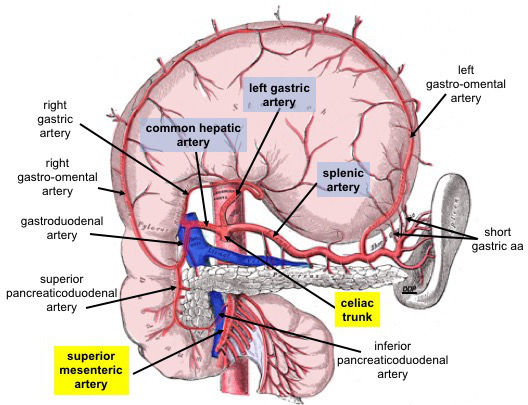
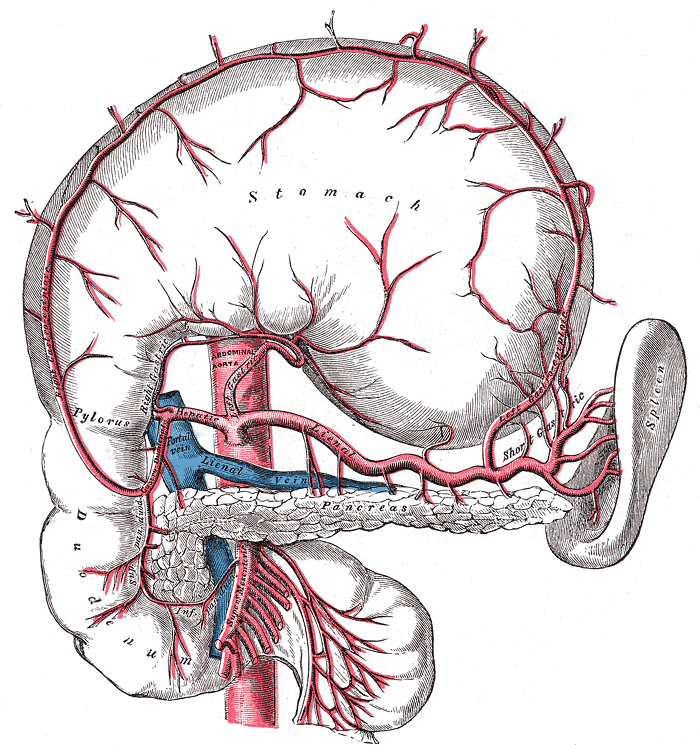
The celiac trunk exits the aorta at T12, immediately below the aortic hiatus. It trifurcates into left gastric, splenic, and common hepatic.
Runs along the lesser curvature of the stomach. Gives off esophageal branches to the distal esophagus before turning along the stomach.
Runs along the superior border of the pancreas (tortuous path). Gives off short gastric arteries and the left gastroepiploic artery before reaching the splenic hilum.
Splits into the gastroduodenal artery (GDA) and the proper hepatic artery. The proper hepatic then gives off the right gastric and divides into right and left hepatic arteries. The cystic artery branches from the right hepatic.
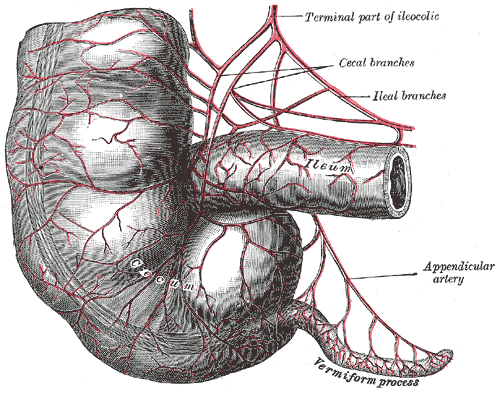
Eliminate the wrong arteries. Which vessel supplies each gut segment?
Areas between two arterial territories that are vulnerable to ischemia during hypotension.
Where the SMA territory (middle colic, via marginal artery) meets the IMA territory (left colic). This is the most common site of ischemic colitis in hypotensive patients.
Where the superior rectal artery (terminal IMA) meets the middle and inferior rectal arteries (internal iliac). Second most common watershed zone.
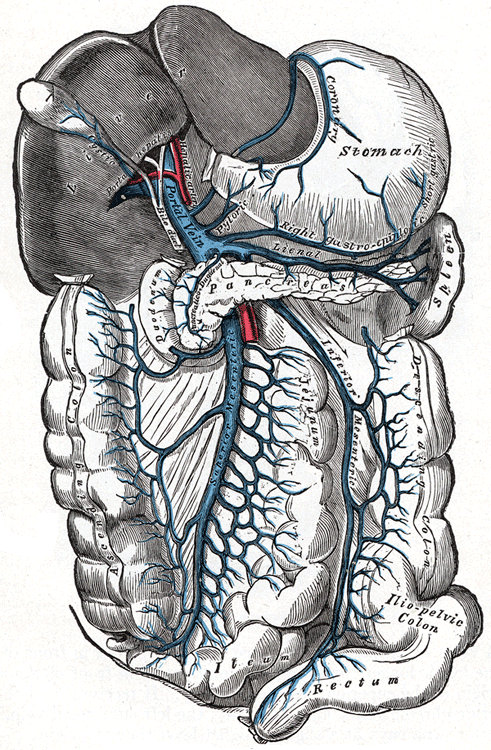
When portal pressure rises, blood detours through connections between the portal and systemic venous systems. The four classic sites:
49 clinical vignettes. Answers shuffle each round. Right-click or long-press to cross out options. Double-tap to highlight.
