Eight tests. Each one a specific question you're asking the patient's body. Know the question, know the answer.
A 34-year-old rock climber presents with pain and tingling radiating down the right arm after a fall. You extend and sidebend the cervical spine toward the painful side, then apply an axial load. The patient reports sharp pain shooting into the right C6 dermatome.
Which test did you just perform?
Adson Test
Spurling Test
Wallenberg Test
Apley Scratch Test
Spurling Test = cervical compression maneuver. Extend + sidebend + axial load. The combination narrows the neural foramen, reproducing radicular symptoms if a nerve root is compressed. The dermatome pattern tells you which level.
Extensor compartments: 1st = APL + EPB (de Quervain)
Spurling Test▾
Cervical
Tests For
Cervical radiculopathy (nerve root compression)
How To Perform
Extend the neck, sidebend toward the symptomatic side, then apply axial compression (push down on the head).
Positive Finding
Reproduces radicular pain down the arm in the affected dermatome.
Three moves in sequence: extend, sidebend, compress. You're shrinking the neural foramen to see if the nerve screams.
Adson Test▾
TOS
Tests For
Thoracic Outlet Syndrome via anterior scaleneThe anterior scalene runs from the transverse processes of C3-C6 to the first rib. The subclavian artery and brachial plexus pass between the anterior and middle scalenes. compression.
How To Perform
Turn head TOWARD the affected side, extend the neck, deep breath in. Palpate the radial pulse throughout.
Positive Finding
Diminished or absent radial pulse on the affected side.
Adson = "Add-toward." Head turns TOWARD. The scalene tightens and pinches the subclavian artery against the first rib.
Wright Test▾
TOS
Tests For
Thoracic Outlet Syndrome via pectoralis minorPec minor attaches to ribs 3-5 and the coracoid process. The neurovascular bundle passes deep to it. Hyperabduction stretches the bundle over the muscle. compression.
How To Perform
Hyperabduct the arm overhead (full abduction past 90 degrees). Palpate the radial pulse.
Positive Finding
Diminished or absent radial pulse.
Wright = "Right up." Arm goes straight up. Pec minor catches the neurovascular bundle like a clothesline.
Military Posture Test▾
TOS
Tests For
Thoracic Outlet Syndrome via costoclavicular spaceThe costoclavicular space is the narrow gap between the clavicle and the first rib. Drawing the shoulder down and back closes that gap and pinches the subclavian vessels and brachial plexus inside it. compression. Also called the Costoclavicular test.
How To Perform
Patient stands at attention: draw the shoulders DOWN and BACKWARD while depressing and extending the shoulder. Palpate the radial pulse throughout.
Positive Finding
Diminished or absent radial pulse on the affected side.
Military = "attention!" Chest out, shoulders down and back. The collarbone clamps onto the first rib and chokes the subclavian in the costoclavicular vise.
Wallenberg Test▾
Cervical
Tests For
Vertebral artery insufficiency. A safety screening test.
How To Perform
Extend and rotate the cervical spine. Hold for several seconds.
Positive Finding
Dizziness, nystagmus, visual changes (the 5 D's and 3 N's).
CRITICAL: this test must be performed BEFORE cervical HVLA. A positive Wallenberg = absolute contraindication to cervical thrust. You could cause a stroke.
Crossed Straight Leg Raise▾
Low Back
Tests For
Lumbar radiculopathy from a large central disc herniation (highly specific).
How To Perform
Raise the asymptomatic (good) leg straight, knee extended.
Positive Finding
Pain reproduced in the opposite (symptomatic) leg.
Lift the GOOD leg and the BAD leg screams. Only a big central disc does that, so it is far more specific than a plain SLR.
Psoas Tension Test▾
Low Back
Tests For
A tight iliopsoas driving lumbar somatic dysfunction.
How To Perform
Patient prone. Flex the knee to 90 degrees, grasp the thigh, and extend the hip until the ASIS lifts off the table. Compare sides.
Positive Finding
Restricted range or quality of hip extension on the tight side.
Lift the thigh off the table: a tight psoas stops it short and tugs the ASIS up early.
Hip Drop Test▾
Sacrum/Pelvis
Tests For
Lumbar and thoracolumbar sidebending.
How To Perform
Patient standing. Monitor iliac crest heights while they bend one knee, keeping that heel on the floor.
Positive Finding
Normal = the lumbar spine curves toward the opposite side and the ipsilateral crest drops more than 20 to 25 degrees. Failure of that crest to drop = lost sidebending on that side.
Bend the knee, heel stays down: the hip should drop and the spine curve away. No drop = stuck sidebending there.
Pelvic Side Shift Test▾
Sacrum/Pelvis
Tests For
Whether the sacrum sits midline.
How To Perform
Patient standing, physician behind. Stabilize one shoulder and translate the pelvis toward that side, then repeat the other side.
Positive Finding
Positive toward the side of freer translation (the pelvis slides more easily that way).
The pelvis slides easier toward the dysfunction. Trap: a RIGHT psoas drives a positive shift to the LEFT.
Lumbosacral Spring Test▾
Sacrum/Pelvis
Tests For
A sacral base held posterior.
How To Perform
Patient prone. Place the heel of the hand over the lumbosacral junction and spring it anteriorly.
Positive Finding
Little or no spring = sacral base posterior (also positive with bilateral or unilateral sacral extension and a backward torsion).
No give means the base is stuck back. A springy L5 on S1 is the normal, healthy feel.
Sphinx Test (Backward Bending)▾
Sacrum/Pelvis
Tests For
Sorting a sacral base held anterior vs posterior.
How To Perform
Patient prone, thumbs in the sacral sulci. Have them prop up on the elbows (the sphinx position) and recheck the sulci.
Positive Finding
If the depth difference worsens, the shallow side is held posterior; if it evens out, the deeper side was held anterior.
Prop up like a sphinx: worse asymmetry blames the shallow (posterior) side, better symmetry blames the deep (anterior) side.
Ober's Test▾
Sacrum/Pelvis
Tests For
A tight tensor fascia lata or iliotibial band.
How To Perform
Patient side-lying on the opposite side. Abduct and slightly extend the hip with the knee bent, then release the leg.
Positive Finding
The thigh stays up in abduction instead of dropping toward the table.
A tight IT band will not let the leg fall.
Thomas Test▾
Sacrum/Pelvis
Tests For
A hip flexor (iliopsoas) contracture.
How To Perform
Patient supine, hugging both knees to the chest, then lowers one leg at a time toward the table.
Positive Finding
The lowered thigh lifts off the table (lumbar lordosis increases) on the tight side.
Hug both knees, drop one: a tight psoas tents that thigh up off the table.
Patrick Test (FABERE)▾
Sacrum/Pelvis
Tests For
Hip joint vs sacroiliac joint pathology (classically hip osteoarthritis).
How To Perform
Supine figure-4: Flexion, ABduction, External Rotation, Extension, while stabilizing the opposite ASIS.
Positive Finding
Anterior groin pain = hip joint; posterior pain = SI joint.
FABER spells the moves. Groin pain points to the hip, buttock pain points to the SI joint.
Apley Compression Test▾
Knee
Tests For
A meniscal tear.
How To Perform
Patient prone, knee flexed to 90 degrees. Press straight down through the heel while rotating the tibia in and out.
Positive Finding
Pain with the downward grind.
Compress and grind the meniscus: push DOWN and it hurts = meniscus.
Apley Distraction Test▾
Knee
Tests For
Collateral ligament injury (MCL or LCL).
How To Perform
Patient prone, knee flexed to 90 degrees. Pull the foot upward (distraction) while rotating the tibia in and out.
Positive Finding
Pain with traction.
Pull UP to unload the meniscus, so now pain = ligament, not meniscus. Compression vs distraction is the whole trick.
Lachman Test▾
Knee
Tests For
ACL integrity (the most sensitive ACL test).
How To Perform
Supine, knee flexed 20 to 30 degrees. Hold the distal femur and pull the proximal tibia forward.
Positive Finding
Excessive anterior glide with a soft, mushy endpoint.
Small bend, pull the shin forward: a torn ACL feels like a drawer that slides with no stop.
McMurray Test▾
Knee
Tests For
A posterior meniscus tear.
How To Perform
Supine, fully flex the knee with a hand on the joint line. External rotation + valgus then extend (medial meniscus), or internal rotation + varus (lateral meniscus).
Positive Finding
A palpable or audible click with pain.
External rotation + valgus = medial; internal + varus = lateral. The click is the torn flap catching.
The tibia slides forward out from under the femur.
90-degree pull-forward = ACL. Lachman is the more sensitive cousin.
Posterior Drawer Test (Knee)▾
Knee
Tests For
The PCL.
How To Perform
Same 90-degree setup. Push the tibia backward.
Positive Finding
The tibia sags or slides backward.
Push back = PCL.
Finkelstein Test▾
Wrist
Tests For
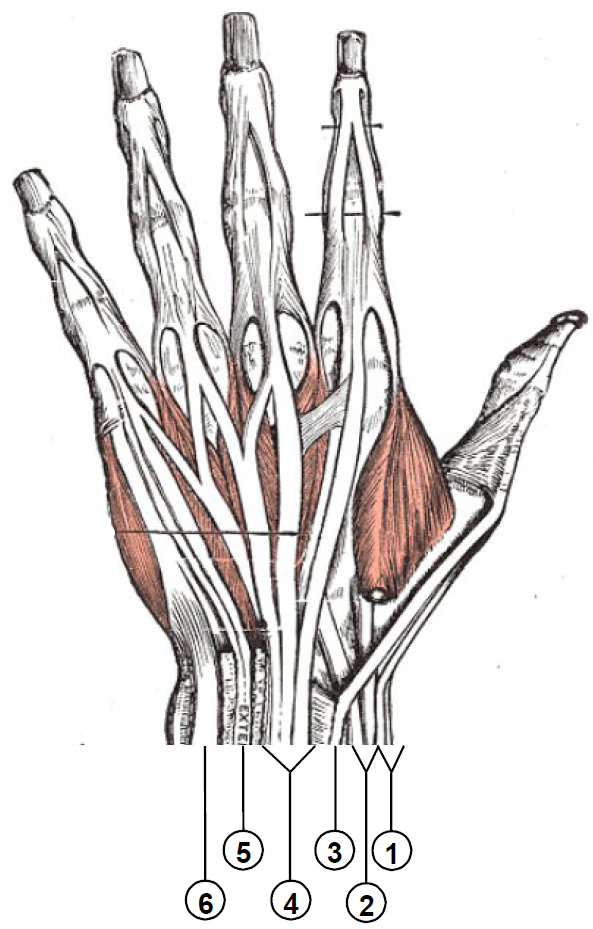
De Quervain tenosynovitis (inflammation of the APL and EPBAbductor Pollicis Longus and Extensor Pollicis Brevis. These two tendons share the first dorsal compartment of the wrist. They pass over the radial styloid. tendons).
How To Perform
Tuck the thumb into a closed fist, then ulnar deviate the wrist.
Positive Finding
Sharp pain over the radial styloid.
New mother with wrist pain from holding the baby = De Quervain. Finkelstein confirms it. The fist + ulnar deviation stretches the inflamed tendons over the radial styloid like a bowstring.
Finkelstein Test
Fist + Ulnar Deviation
1st Compartment: APL + EPB
Tinel Sign (Wrist)▾
Wrist
Tests For
Carpal tunnel syndrome · compression of the median nerve at the wrist. A nerve test, not a tendon test like Finkelstein.
How To Perform
Tap (percuss) lightly over the median nerve at the volar wrist crease, right over the carpal tunnel.
Positive Finding
Electric tingling that shoots into the thumb, index, middle, and the radial half of the ring finger.
Tinel = Tap. Tap the nerve, light up the fingers. If percussing the wrist sends lightning into the first three and a half fingers, the median nerve is irritated. Tinel also works at the elbow for the ulnar nerve.
Phalen Test▾
Wrist
Tests For
Carpal tunnel syndrome · median nerve compression. Same target as Tinel, different maneuver.
How To Perform
Press the backs of both hands together with the wrists fully flexed and fingers pointing down (the "backwards prayer"), and hold about 60 seconds. Flexing the wrist squeezes the carpal tunnel.
Positive Finding
Tingling or numbness in the median distribution: thumb, index, middle, radial half of the ring finger.
Backwards prayer, hold a minute. Wrist flexion narrows the tunnel and pinches the median nerve. Reverse Phalen is the same idea with the palms together and wrists extended. Either way you crush the tunnel and reproduce the tingling.
Apley Scratch Test▾
Shoulder
Tests For
Rotator cuff ROM: evaluates multiple cuff muscles in two motions.
How To Perform
Hand behind head (external rotation + abduction) tests supraspinatus and infraspinatus. Hand behind back (internal rotation + adduction) tests subscapularis.
Positive Finding
Inability to reach or pain during either motion indicates the corresponding cuff muscle is compromised.
The only test on this list that's TWO motions in one. Hand UP behind head = external rotators. Hand DOWN behind back = internal rotator (subscapularis).
Drop Arm Test▾
Shoulder
Tests For
Full-thickness rotator cuff tear, specifically the supraspinatusSupraspinatus starts abduction (the first 15 degrees) and helps hold the arm out to the side. A full-thickness tear leaves nothing to control the arm on the way down from abduction.. Also called the Codman test.
How To Perform
Passively abduct the arm to about 90 degrees (or full abduction), then ask the patient to slowly lower it back to the side.
Positive Finding
The arm drops suddenly or cannot be lowered smoothly, often giving out around 90 degrees.
Drop Arm = the rope is cut. Supraspinatus is torn, so on the way down nothing holds the arm. It just drops. Dead weight at about 90 degrees. Apley screens ROM, Drop Arm catches the tear.
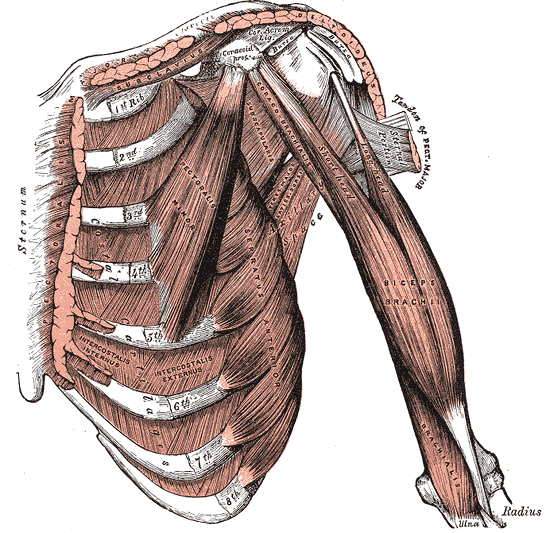
Patient performs resisted forward flexion with the elbow fully extended and forearm supinated.
Positive Finding
Pain in the bicipital groove (anterior shoulder).
Speed = Straight arm. Elbow extended, forearm supinated, push up against resistance. The long head of biceps is loaded at its groove.
Yergason Test▾
Shoulder
Tests For
Biceps tendon pathology AND bicipital groove stability: the integrity of the transverse humeral ligamentThe transverse humeral ligament is the strap that roofs the bicipital groove and holds the long head of the biceps tendon inside it. If it tears, the tendon can sublux (snap) out of the groove. that keeps the long head of the biceps tendon seated in its groove.
How To Perform
Elbow flexed at 90 degrees. Patient attempts resisted supination of the forearm (often with external rotation).
Positive Finding
Pain in the bicipital groove points to tendinitis. A palpable pop or snap as the tendon jumps out of the groove means the transverse humeral ligament is torn (instability).
Yergason = Yer-turn-yer-palm-up. Resist supination at 90 degrees. Pain = inflamed tendon. A pop = the tendon escaping the groove because its ligament roof gave out. Speed loads the tendon with flexion, Yergason checks the groove with supination.
Tests by Region
Grouped by where on the body you're testing.
Cervical
Shoulder · Upper Extremity
Wrist · Hand
Two cervical tests, two completely different goals. Spurling asks: "Is there nerve root compression?" Wallenberg asks: "Is it safe to manipulate this neck?"
Maneuver: Extend + sidebend toward symptomatic side + axial load. This narrows the neural foramenThe opening between adjacent vertebrae where the spinal nerve root exits. Disc herniation or osteophytes can narrow this space and compress the nerve..
Positive: Reproduces the patient's radicular symptoms (pain, numbness, or tingling radiating into the arm).
Maneuver: Extend + rotate the cervical spine. Hold position. This kinks the vertebral arteryRuns through the transverse foramina of C1-C6. Extension + rotation can compress it against bone, reducing posterior circulation to the brainstem and cerebellum..
Positive: Dizziness, nystagmus, visual disturbances, drop attacks, dysarthria. ANY positive sign = do NOT perform cervical HVLA.
Board trap: Spurling sidebends TOWARD the affected side (closing the foramen). A question might try to trick you with "away from" the symptomatic side. Wallenberg is a prerequisite for HVLA: always test BEFORE you thrust.
Five tests in this region. Two for TOS (Adson, Wright), one for rotator cuff ROM (Apley Scratch), and two for biceps tendon (Speed, Yergason).
Adson Test
Target: TOS via anterior scalene compression
Maneuver: Head TOWARD the affected side + extend neck + deep breath. The anterior scalene contracts, compressing the subclavian artery against the first rib.
Positive: Diminished radial pulse on the tested side.
Wright Test (Hyperabduction)
Target: TOS via pectoralis minor compression
Maneuver: Arm hyperabducted overhead past 90 degrees. The neurovascular bundle stretches over the pec minor tendon at the coracoid.
Positive: Diminished radial pulse.
Apley Scratch Test
Target: Rotator cuff ROM (supraspinatus, infraspinatus, subscapularis)
Maneuver: Two parts. (1) Hand behind head: external rotation + abduction. (2) Hand behind back: internal rotation + adduction.
Positive: Inability or pain with either motion. Behind-head = external rotators (supraspinatus, infraspinatus). Behind-back = internal rotator (subscapularis).
Positive: Pain in the bicipital groove (anterior shoulder).
Yergason Test
Target: Biceps tendon pathology
Maneuver: Resisted supination with elbow at 90 degrees.
Positive: Pain in the bicipital groove.
Speed vs. Yergason: Both target the bicipital groove, but the arm positions are different. Speed = straight arm, resist flexion. Yergason = bent elbow, resist supination. in clinical practice, the maneuver description tells you which test they mean.
One test here, but it's a board favorite. The classic presentation is a new mother with radial-sided wrist pain.
Maneuver: Thumb tucked inside a closed fist, then ulnar deviate the wrist. This stretches the APL and EPB tendons over the radial styloid.
Positive: Sharp pain over the radial styloid process.
Classic stem: "A 28-year-old woman with a 3-month-old infant presents with wrist pain worse with gripping." The repetitive thumb abduction from holding the baby inflames the first dorsal compartment. Finkelstein confirms.
Elimination Game
Read the vignette. Reveal clues one at a time. Eliminate tests that don't fit.
A 42-year-old guitar player presents with numbness and tingling in the right hand. She reports the symptoms are worst when she sleeps with her arm above her head. On exam, you notice her symptoms reproduce when you position her arm in a specific way while monitoring her pulse.
Spurling Test
Adson Test
Wright Test
Finkelstein Test
Speed Test
Clue 1: The symptoms involve the hand, not the neck. The patient doesn't have neck pain or radicular symptoms. This rules out cervical radiculopathy.
Clue 2: The symptoms reproduce when the arm is overhead. The exam involves monitoring the radial pulse. This is a vascular compression test.
Clue 3: Symptoms worst with arm above head = the structure being compressed is under the pectoralis minor, not the anterior scalene. Adson tests the scalene (head turn), not overhead positioning.
Clue 4: Finkelstein tests wrist tendons (De Quervain). Speed tests biceps tendon. Neither involves pulse monitoring. Both eliminated.
Wright Test (Hyperabduction). The arm-overhead position compresses the neurovascular bundle under pectoralis minor. The guitarist's habit of sleeping with arms overhead reproduces TOS symptoms. Diminished radial pulse with hyperabduction confirms pec minor compression.
A 55-year-old man with chronic neck pain is scheduled for osteopathic manipulation. Before performing cervical HVLA, you need to complete a safety screen. You position the patient's head in a specific way and observe for neurological signs.
Spurling Test
Wallenberg Test
Adson Test
Yergason Test
Apley Scratch
Clue 1: This is a SAFETY screen before HVLA. That word "safety" narrows it immediately. Only one test on this list is specifically a pre-HVLA safety test.
Clue 2: You're watching for neurological signs (dizziness, nystagmus, visual changes). Not radicular pain, not pulse changes, not tendon pain.
Clue 3: Yergason and Apley Scratch test shoulder structures. They have nothing to do with cervical safety screening. Eliminated.
Clue 4: Adson tests TOS (pulse monitoring). Spurling tests nerve root compression. Neither is a pre-manipulation safety screen for vertebral artery compromise.
Wallenberg Test. Extend + rotate the cervical spine and watch for dizziness, nystagmus, or visual changes. A positive Wallenberg = the vertebral artery is being compromised = absolute contraindication to cervical HVLA. You could cause a vertebrobasilar stroke.
clinical Walkthrough
Full vignettes with clue highlights. Pick your answer, then walk through every option.
QUESTION 1 OF 25
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated June 30, 2026 at 2:05 AM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.