Ribs move with breathing. When they get stuck, the motion tells you everything. Learn the mechanics, nail the diagnosis.
Opening Challenge
A patient cannot fully breathe out on the right. On structural examination, rib 6 on the right moves well during inhalation but fails to descend during exhalation. The rib appears held in its elevated (inhaled) position at rest.
What is the correct somatic dysfunction diagnosis?
Correct: B, Inhalation dysfunction. A rib is named for the position it is held in (the direction it moves freely), not the direction it is blocked from. This rib moves freely into inhalation (rises fine) but fails to descend on exhalation. It is held in the inhaled, elevated position, so the diagnosis is an inhalation dysfunction. It happens to be restricted in exhalation, but that blocked motion is not what names it.
Common trap: "It cannot exhale, so it must be an exhalation dysfunction." That names the rib off the blocked direction, which is backwards. Name it off where it is stuck and what it prefers: held up, prefers inhalation, equals inhalation dysfunction. Think of a turnstile jammed in one position: you describe where it is stuck, not the direction it refuses. Break it down: name the rib for the position it is held in. Held UP (inhaled) = inhalation dysfunction; held DOWN (exhaled) = exhalation dysfunction. Key rib by BITE: Bottom Inhaled, Top Exhaled.
scroll to learn
Section 1
How Ribs Move
Ribs rotate around different axes depending on their position. Three distinct motion types. Know which group does which and you can answer any mechanics question cold.
Pump handle · ribs 1 to 5
The anterior rib ends rise during inhalation and fall during exhalation. That forward lift increases anterior posterior chest diameter.
What will you do next time? Upper anterior chest clue → pump handle group → ribs 1 to 5.
Most commonly tested rib motion in OMM exams. The diaphragmatic ribs (6-10) rely on this motion for the majority of respiratory excursion.
Ribs 11-12
Caliper
Attachment: costovertebral articulation only, no anterior attachment (floating ribs).
Motion: the free tips flare outward on inhalation and move inward on exhalation, like caliper jaws opening and closing.
Dysfunction here affects respiratory diaphragm mechanics, as well as psoas and quadratus lumborum attachments.
●
Rule of 3s: Ribs 1-5 = pump handle (anterior end moves). Ribs 6-10 = bucket handle (lateral middle moves). Ribs 11-12 = caliper (tips flare). The groupings match the anatomical lever arm. Memorize the number ranges once and you never confuse motion types again.
Section 2
Somatic Dysfunction Naming
The naming rule is the single most tested concept in rib OMM. Get this right and half the questions answer themselves.
Inhalation Dysfunction
Stuck UP
Position: rib is held in the inhaled (elevated) position
Exam finding: rib fails to rise during the inhalation phase (moves less cephalad)
Key rib in a group: HIGHEST rib (Top Exhaled)
KEY RIB = HIGHEST
⚠
The naming rule: A rib is named for the position it is held in (the direction it moves freely, its ease), not the direction it is blocked from. A rib held UP in the inhaled position (free to inhale, stuck against exhalation) is an inhalation dysfunction; a rib held DOWN in the exhaled position is an exhalation dysfunction. Key rib mnemonic: BITE · Bottom Inhaled, Top Exhaled. Naming off the blocked motion ("it cannot exhale, so call it exhalation") is the #1 wrong answer in clinical practice.
Inhalation Dysfunction
Treatment Approach
Rib is held up (inhaled position), restricted from descending.
Goal: restore exhalation, get the rib to come DOWN.
MET (post-isometric relaxation): the physician holds the key rib toward exhalation. Patient instruction: INHALE against resistance, contracting the scalene (the muscle holding the rib up); after the 3-5 second isometric effort the patient relaxes and the rib settles further down on the release. A passive exhale (respiratory assist) is not the move here.
Key rib: lowest in the group. Treat the lowest first.
Exhalation Dysfunction
Treatment Approach
Rib is held down (exhaled position), restricted from rising.
Goal: restore inhalation, get the rib to come UP.
MET (muscle moves bone): the physician supports the key rib as the patient INHALES against resistance; the segmental muscle (scalenes for ribs 1-2, pec minor 3-5, serratus anterior 6-9, latissimus dorsi and QL 10-12) contracts and lifts the rib toward inhalation.
Key rib: highest in the group. Treat the highest first.
Section 3
Key Ribs and High-Yield Groups
Certain ribs are tested repeatedly. Rib 1 is the most tested. Know what makes each high-yield rib special clinically.
Rib
Motion Type
Clinical High-Yield
Key Rib Rule
Rib 1
Pump Handle
Inhalation dysfunction = held UP. Scalene hypertonicity holds it elevated. Can compress brachial plexus and subclavian vessels (thoracic outlet-like). Adson test positive.
Treat rib 1 directly; scalene post-isometric relaxation with contralateral cervical sidebending to let it descend
Rib 2
Pump Handle
Posterior scalene attaches to rib 2. Commonly elevated with rib 1 in respiratory illness (inhalation dysfunction, held up).
Highest = key rib in an exhalation-dysfunction group; lowest = key in an inhalation-dysfunction group
Ribs 2-5
Pump Handle
Group inhalation dysfunction: ribs held up, restricted from descending. Evaluate AP (pump-handle) excursion at the upper chest.
LOWEST = KEY for inhalation group; HIGHEST = KEY for exhalation group
Ribs 11-12
Caliper
Free-floating ribs. No anterior attachment. Dysfunction affects diaphragm, psoas, and quadratus lumborum. Often involved in low back pain and breathing pattern disorders.
Treat each individually; no costal cartilage to guide group mechanics
Rib 1 · Most Tested
Inhalation Dysfunction
Held up, cannot descend. The anterior and middle scalene muscles attach to the superior surface of rib 1. Scalene hypertonicity (stress, infection, cervical dysfunction) pulls rib 1 cephalad and holds it elevated, so it is held in the inhaled position and restricted from descending.
Symptoms: arm numbness, tingling (brachial plexus), venous congestion in the arm, positive Adson test.
Treatment: scalene post-isometric relaxation, rib 1 MET with contralateral cervical sidebending against resistance to let the rib descend. The scalene muscles are the target, not just the rib.
Group Dysfunction · Bucket Handle
Ribs 6-10 Example
Ribs 7, 8, and 9 all fail to descend on exhalation (held up). This is a group inhalation dysfunction.
Key rib: the LOWEST restricted rib = rib 9.
Treat rib 9 first with post-isometric relaxation: physician holds rib 9 toward its exhalation position, patient inhales against resistance to contract the holding muscle for 3-5 seconds then relaxes, repeat 3-5 cycles, take up slack. Releasing the lowest rib typically frees the group above it.
Anatomy Check
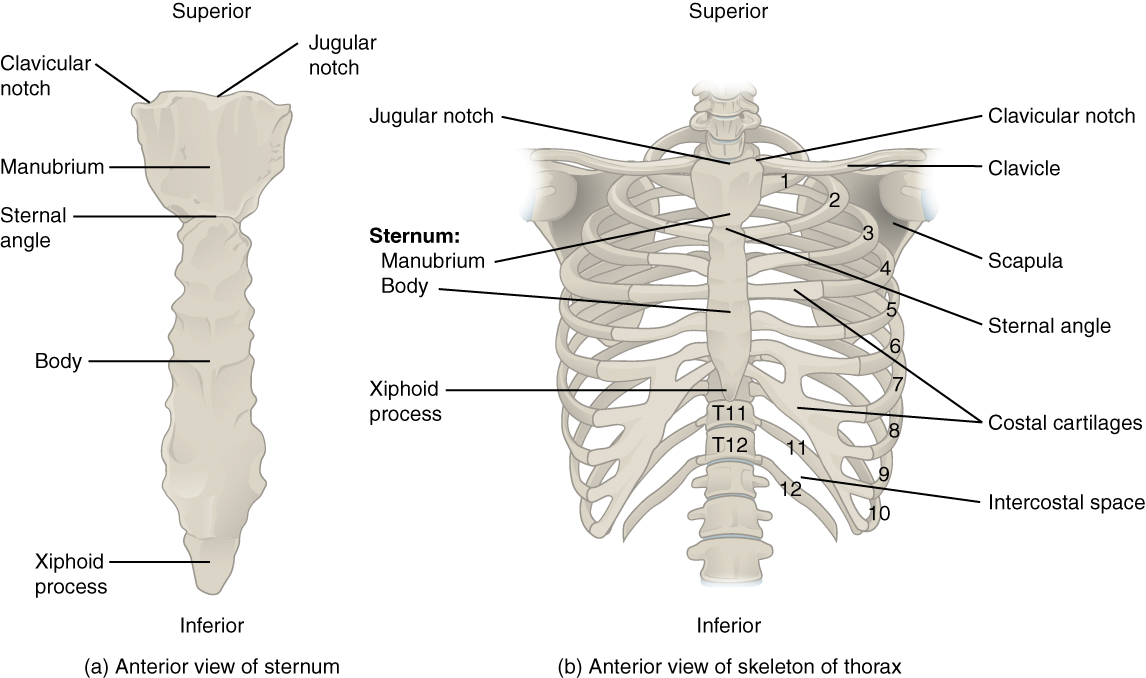
Thoracic cage landmarks
Use the images to keep the motion rules tied to the actual lever arms: upper anterior ribs pump, middle lateral ribs bucket, floating ribs caliper.
Rib cage overview. Upper ribs attach near the sternum, so the anterior ends drive pump-handle motion.Single rib landmarks. The angle and tubercle are the contact landmarks that make motion testing clinically useful.Costovertebral joints. Posterior articulation explains why rib dysfunction is tested through respiratory motion, not just pain location.
Section 4
Treatment Techniques
MET is the primary tool. Know the patient instruction for each dysfunction type and you can work backwards to any answer choice.
MET · Inhalation Dysfunction
Patient INHALES, then relaxes
Rib is held up. Goal: get it to descend (restore exhalation).
1. Physician holds the rib toward its exhalation (lowered) position.
2. Instruction to patient: "Breathe IN against my hand" to fire the scalene, then relax.
3. Patient exerts force for 3-5 seconds isometrically, then relaxes.
4. On relaxation, physician takes the rib to its new lowered position.
5. Repeat 3-5 cycles. Re-examine.
Rationale: post-isometric relaxation lengthens the muscle holding the rib up, letting the rib descend further with each cycle.
MET · Exhalation Dysfunction
Patient INHALES
Rib is held down. Goal: get it to rise (restore inhalation).
1. Physician supports the rib toward its inhalation (elevated) position.
2. Instruction to patient: "Breathe IN against my hand."
3. Patient inhales isometrically for 3-5 seconds. The segmental rib-elevating muscle contracts.
4. On the effort the muscle lifts the rib; physician takes up slack toward elevation.
5. Repeat 3-5 cycles. Re-examine.
Rationale: muscle-moves-bone, the rib's segmental muscle (scalenes 1-2, pec minor 3-5, serratus 6-9, lat/QL 10-12) actively lifts the depressed rib.
Direct HVLA · Rib Thrust
Costovertebral Gapping
High-velocity, low-amplitude thrust over the angle of the rib to gap the costovertebral joint.
Position: prone or lateral recumbent.
Absolute contraindications: osteoporosis, rib fracture or metastatic disease to ribs and vertebrae, bleeding disorder, anticoagulation therapy.
Used when the dysfunction is acute, well-localized, and the patient can tolerate the technique. Not first-line for chronic or multi-rib dysfunction.
Respiratory Assistance
Indirect Technique
Physician places hands over the rib. Patient breathes normally.
During the corrective phase (exhalation for an inhalation dysfunction, inhalation for an exhalation dysfunction), the physician provides gentle traction and guidance to encourage normal rib excursion.
Use when: direct technique is too aggressive, acute pain, elderly patient, post-surgical, or patient cannot perform isometric contraction (sedated, neurologically impaired).
Works by reinforcing normal physiologic motion rather than correcting against restriction.
●
MET rule for ribs: Both dysfunctions work the rib's segmental (inhalation) muscle; the technique is what differs. Exhalation dysfunction (held down): muscle moves bone, the patient inhales and the muscle actively lifts the rib up. Inhalation dysfunction (held up): post-isometric relaxation, the patient contracts that muscle against resistance (a brief inhale effort), then relaxes, and the rib drops down on the release. Key rib by BITE: Bottom Inhaled, Top Exhaled.
Section 5 · Elimination Game
Find the Key Rib
Work through the clues. Each one eliminates wrong answers until only the correct diagnosis remains. Tap a clue to reveal it, then eliminate the cards that contradict it.
A 45-year-old woman presents with right-sided chest tightness and reduced breath sounds at the right base. On structural examination, ribs 7, 8, 9, and 10 on the right all demonstrate the same finding: during inhalation they move freely upward, but during exhalation they fail to descend normally on the right (they move less caudad than the left). The left side is normal. The physician needs to record the diagnosis and identify the key rib for treatment.
The ribs move freely on INHALATION but fail to DESCEND on EXHALATION. They are held in the inhaled (elevated) position. A rib is named for the position it is held in, so this is an inhalation dysfunction. Eliminate any answer labeled "exhalation dysfunction."
For a group with INHALATION dysfunction (ribs held UP, restricted from descending), the key rib is the LOWEST rib in the group (Bottom Inhaled). The involved ribs are 7, 8, 9, and 10. The lowest = rib 10. Eliminate any answer that lists rib 7 as the key rib.
The ribs are held up and cannot descend on exhalation = held in the inhaled position = inhalation dysfunction. For a group with inhalation dysfunction, treat the LOWEST rib first. Rib 10 is the key rib.
Treatment (post-isometric relaxation): physician holds rib 10 toward its exhalation position. Patient inhales against resistance to contract the holding muscle for 3-5 seconds, then relaxes so the rib settles further down. Physician takes up the new slack. Repeat 3-5 cycles, then reassess all four ribs.
Section 6 · DO-Style Practice
Clinical Questions
Eight original DO/clinical questions. Work through each vignette before tapping an answer.
1 / 8
During a structural examination, a physician finds that a patient's rib 8 on the left moves freely upward during inhalation but does not descend during exhalation. When asked to take a deep breath, rib 8 rises normally. When asked to blow out fully, rib 8 remains elevated.
How should this dysfunction be recorded in the medical chart?
Correct: A, Inhalation dysfunction, rib 8 left. The rib is held in the INHALED (elevated) position: it rises freely on inhalation but fails to descend on exhalation. A rib is named for the position it is held in (its free direction), so this is an inhalation dysfunction. It is restricted in exhalation, but that blocked motion does not name it.
B is wrong: that names the rib off the blocked exhalation, which is backwards. Held up in the inhaled position = inhalation dysfunction. C is wrong: same naming error, plus the matching wrong treatment. D is wrong: bucket-handle is a motion type, not a dysfunction direction, and the rib is held elevated, not lowered. Good instinct if you reached for the blocked motion: it cannot exhale, so "exhalation" feels right. The naming runs the other way: name the rib for where it is stuck and what it prefers. Held up, prefers inhalation, equals inhalation dysfunction. Think of a recliner jammed fully reclined: you describe where it is stuck (reclined), not the direction it refuses. Break it down: held UP in the inhaled position = inhalation dysfunction (restricted in exhalation); held DOWN in the exhaled position = exhalation dysfunction (restricted in inhalation); name it for the held position, not the block.
Treatment: post-isometric relaxation. The physician holds rib 8 toward exhalation; the patient INHALES against resistance to contract the muscle holding the rib up, then relaxes, and the rib settles further down on each release.
2 / 8
A physician is treating a patient with group rib dysfunction. Ribs 3, 4, and 5 on the right all fail to descend during exhalation. Each rib stays in its inhaled (elevated) position during quiet breathing. The patient has reduced right-sided respiratory excursion at the upper chest.
Which rib should be treated first, and what is the correct MET patient instruction?
Correct: D, Rib 5 first; patient inhales against resistance.
Group inhalation dysfunction: ribs 3, 4, and 5 are all held in the inhaled (elevated) position, restricted from descending. A rib is named for the position it is held in, so this is an inhalation dysfunction.
Key rib: for a group with inhalation dysfunction, the key rib is the LOWEST rib = rib 5 (Bottom Inhaled). Treat rib 5 first. Releasing it typically frees the ribs above it.
MET instruction (post-isometric relaxation): the physician holds rib 5 toward its exhalation position; the patient INHALES against resistance to contract the muscle holding the rib up, then relaxes, and the rib settles further down on the release. Repeat and take up slack toward exhalation.
A is wrong: rib 3 (the highest) is the key rib for EXHALATION dysfunction groups (Top Exhaled), not this inhalation group. B and C are wrong: a passive exhale (respiratory assist) is not the technique for an inhaled rib. You free it with post-isometric relaxation: contract the holding muscle, then relax, and the rib drops on the release. Good instinct on rib 5 as the key rib in B; the trap is the instruction. You do not exhale a stuck-up rib down, you contract the scalene/holding muscle and then relax. Break it down: inhalation dysfunction key rib = LOWEST, treated by post-isometric relaxation (patient inhales to contract, then relaxes, rib descends); exhalation dysfunction key rib = HIGHEST, treated by muscle moves bone (patient inhales, muscle lifts the rib).
3 / 8
A 52-year-old woman is found to have rib 1 on the right in an elevated, anterior position. She reports right arm tingling and a sensation of fullness in her right neck. Structural examination confirms rib 1 cannot descend to its neutral position. Adson's test is positive on the right.
Which muscle's hypertonicity is most likely maintaining this dysfunction?
Correct: B, Right scalene muscles.
This is rib 1 inhalation dysfunction (held UP, cannot descend). The anterior and middle scalenes attach directly to the superior surface of rib 1. Scalene hypertonicity holds rib 1 in the inhaled (elevated) position and prevents it from descending to neutral.
Elevated rib 1 reduces the costoclavicular space, compressing the brachial plexus and subclavian vessels. Adson's test: patient turns head toward the ipsilateral side and inhales while extending the neck. This tightens the scalene and narrows the space further, occluding the subclavian artery (pulse diminishes or disappears).
A is wrong: pectoralis major elevates ribs 2-5 anteriorly, not rib 1. C is wrong: the SCM is a primary mover of the head and neck, not a direct rib 1 elevator in the context of this dysfunction. D is wrong: serratus anterior protracts and upwardly rotates the scapula; it stabilizes the scapula against the thoracic wall but does not elevate or maintain rib 1. The primary accessory exhalation muscles are the internal intercostals and abdominals. Good instinct on the SCM (choice C): it is a prominent neck muscle and it looks like it should anchor rib 1. But the SCM moves the head and neck, not the rib. The scalenes are the dedicated rib 1 lifters, running like guy-wires from the cervical vertebrae down to the top of rib 1. When the guy-wires are too tight, they pull the rib up and hold it there. Break it down: rib 1 inhalation dysfunction (held up) = scalene hypertonicity (anterior and middle scalenes); their attachment to the superior surface of rib 1 prevents descent; Adson's test tightens the scalenes further, confirming the diagnosis.
4 / 8
A patient is positioned supine. The physician places hands under the right posterior thorax at ribs 8-10. The patient is asked to inhale deeply. The physician notes that ribs 8-10 on the right flare laterally during inhalation. During exhalation they return medially. This motion is assessed as full and symmetric with the left side.
What type of rib motion is being assessed, and what does this finding indicate?
Correct: B, Bucket-handle motion; normal lateral diameter expansion.
Ribs 6-10 are the bucket-handle ribs. Their axis of rotation runs anterior-posterior, so the lateral (middle) portion of the rib swings UP and OUT during inhalation, like a bucket handle being lifted sideways. This motion expands the transverse (lateral) diameter of the thorax.
Full symmetric bucket-handle motion at ribs 8-10 = normal respiratory mechanics at this level.
A and D are wrong: pump-handle motion (ribs 1-5) moves the ANTERIOR end up and down, not the lateral middle. Pump handle expands AP diameter, not transverse. Ribs 8-10 are not pump-handle ribs. C is wrong: caliper motion is specific to ribs 11-12, which have no anterior attachment. Ribs 8-10 attach via costal cartilage and cannot perform caliper motion. Good instinct if you chose A or D: pump-handle moves the anterior end, which sounds right for rib motion. But pump-handle belongs only to ribs 1-5, where the short anterior lever arm dominates. Think of the Rule of 3s as three postal districts: 1-5 is pump-handle district, 6-10 is bucket-handle district, 11-12 is caliper district. Ribs 8-10 will never receive pump-handle mail no matter how confidently you address the envelope. Break it down: ribs 1-5 = pump-handle (anterior end moves, AP diameter); ribs 6-10 = bucket-handle (lateral middle moves, transverse diameter); ribs 11-12 = caliper (tips flare, floating ribs only); confusing districts is the #1 rib motion board error.
5 / 8
A 34-year-old woman presents with right arm numbness, tingling in the right fourth and fifth fingers, and mild venous congestion in the right forearm. Structural examination reveals rib 1 on the right in an elevated position, unable to descend to neutral. She has a positive Adson's test on the right.
Which MET instruction is correct for treating this dysfunction?
Correct: C, inhale against resistance while the physician depresses rib 1.
This is rib 1 inhalation dysfunction (held UP, cannot descend). The scalene muscles hold it elevated. It is freed with post-isometric relaxation: the patient INHALES against resistance to contract the scalene, the physician resists isometrically, and on the relaxation that follows the physician carries rib 1 down toward exhalation. Repeat each cycle.
A is wrong: a passive exhale against resistance is respiratory assist, which is not the technique tested for an elevated first rib. You contract the scalene, then use the post-isometric relaxation to let the rib descend. B is wrong: the scalene stretch uses contralateral (not ipsilateral) cervical sidebending, and the rib-focused cue is the contract-then-relax, not a sidebend alone. D is wrong: HVLA is not first-line for rib 1, which sits under the clavicle: direct thrust access is limited and technically risky near the brachial plexus. Break it down: rib 1 inhalation dysfunction (held up) = post-isometric relaxation of the scalene; the patient inhales to contract, then relaxes, and the rib descends; respiratory assist (passive exhale) and HVLA are not the first move here.
6 / 8
On structural examination, ribs 11 and 12 bilaterally do not show the normal outward flaring of their tips during inhalation. The physician notes restricted motion at these ribs that affects the patient's diaphragm mechanics and is correlated with chronic low back pain and restricted lumbar extension.
What type of rib motion do ribs 11 and 12 normally perform, and why are they considered atypical?
Correct: C, caliper motion; floating ribs with costovertebral articulation only.
Ribs 11 and 12 are the floating ribs. They have NO anterior attachment -- no sternum connection, no costal cartilage. Their only articulation is the costovertebral joint at the spine. Because of this, their free tips can only move like caliper jaws: outward on inhalation, inward on exhalation.
Clinically, dysfunction at ribs 11-12 affects the respiratory diaphragm (which attaches here), the psoas major, and the quadratus lumborum. This explains the link to lumbar pain and restricted extension in this vignette.
A is wrong: ribs 1-7 are true ribs that attach directly to the sternum. Pump-handle motion applies to ribs 1-5. B is wrong: ribs 8-10 are false ribs sharing cartilage with rib 7, but they still have indirect anterior attachment and perform bucket-handle motion. Good instinct on choice D (no defined motion): floating ribs seem like they should be clinically irrelevant. They are not. Ribs 11-12 anchor the diaphragm, the psoas major, and the quadratus lumborum, which explains the direct link to lumbar pain and restricted extension in this vignette. Think of ribs 11-12 as the load-bearing struts hidden under a bridge: invisible from the top but holding up everything below. Dysfunction here is not vestigial, it is load-bearing failure. Break it down: ribs 11-12 = floating ribs (costovertebral joint only), caliper motion; dysfunction affects diaphragm + psoas + QL; clinically linked to chronic low back pain and restricted lumbar extension.
7 / 8
A 28-year-old male presents after a motor vehicle accident. Structural exam finds ribs 6, 7, and 8 on the left held in their depressed (exhaled) position and failing to rise on inhalation. The physician identifies this as a group exhalation dysfunction.
Which rib is the key rib and what is the correct next step?
Correct: B, key rib is rib 6 (highest); patient inhales against resistance.
For group EXHALATION dysfunction (ribs held DOWN, cannot rise), the key rib is the HIGHEST rib (Top Exhaled). Here, ribs 6-8 are all held depressed. The highest = rib 6 is the key rib. Treating rib 6 first typically releases the group below it.
MET instruction for exhalation dysfunction (muscle moves bone): the physician supports rib 6 toward its inhalation (elevated) position, then asks the patient to INHALE against resistance for 3-5 seconds; the rib-elevating muscle contracts and lifts the rib, and slack is taken up toward elevation each cycle.
A and D are wrong: rib 8 is correct for INHALATION dysfunction groups (treat the lowest). For exhalation dysfunction, you treat the HIGHEST rib first. C is wrong: rib 6 is correctly identified as the key rib, but exhale against resistance is the instruction for an inhalation dysfunction: the reverse of what is needed here. Good instinct on identifying rib 6: an exhalation dysfunction does use the highest rib. The trap is the direction. The rib is held down and needs to rise, so the patient inhales against resistance and the rib-elevating muscle lifts it (muscle moves bone). Think of working a car jack: each pump of the handle (inhale) raises the load a little higher. Break it down: exhalation dysfunction key rib = HIGHEST (rib 6 here), patient INHALES (muscle moves bone lifts the held-down rib); inhalation dysfunction key rib = LOWEST, patient EXHALES (post-isometric relaxation lets the held-up rib descend).
8 / 8
A 60-year-old woman with severe osteoporosis and a recent diagnosis of metastatic breast cancer to the thoracic spine presents with rib 4 inhalation dysfunction. The osteopath identifies rib 4 as held in the elevated position. The patient is cooperative and can breathe on command.
Which treatment technique is most appropriate here?
This patient has two major contraindications to HVLA: severe osteoporosis and metastatic disease to the thoracic spine. Both are absolute contraindications to direct thrust techniques over the ribs and spine. HVLA in this setting risks rib fracture or pathological vertebral fracture.
MET (choice B) is also riskier in osteoporosis and metastatic disease -- isometric force against a fragile rib cage can fracture ribs. The safest option is respiratory assistance: the physician places gentle hands over rib 4 and guides it downward during exhalation, working WITH the patient's natural respiratory motion rather than against a resistance load.
D is wrong: OMM is not globally contraindicated in cancer. The contraindication is technique-specific: direct force techniques (HVLA, high-load MET) over areas with metastatic involvement. Gentle indirect techniques remain options where clinically appropriate and with patient consent. Good instinct on MET (choice B): isometric techniques are gentler than HVLA. But isometric force applied by the physician against fragile ribs in severe osteoporosis still risks fracture. Respiratory assistance uses only the patient's own breathing momentum, zero added physician force. Think of the difference between lifting a cracked porcelain vase versus guiding it gently to a lower shelf: respiratory assistance is the guiding hand that adds no new force beyond what the patient's breath already generates. Break it down: osteoporosis + metastatic thoracic disease = absolute contraindication to HVLA and high-load MET at affected ribs; respiratory assistance (guiding rib downward with natural exhalation) is the safest technique because no external force is added beyond the patient's own breath.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated July 5, 2026 at 7:52 AM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.