Classic clueFailure to pass meconium in first 48 hours
Board killerAbsent ganglion cells on rectal suction biopsy = Hirschsprung
💡The sweat chlorideNormal: below 30 mmol/L. Borderline: 30-59. CF diagnosis: 60 or above. A result of 22 mmol/L is unambiguously normal and rules out CF and meconium ileus. in this scenario is 22 mmol/L, well below the 40-60 borderline range. This single number kills the CF/meconium ileus diagnosis immediately.
Board Trap: Both Hirschsprung and cystic fibrosis cause a neonate to fail to pass meconium. The sweat chloride is the discriminator. Normal sweat chloride (below 40) means CF is off the table. What is left is Hirschsprung. Confirm with rectal suction biopsy.
1 / 6
The Lineup
RET, the Impostors, and the Critical Contrast
The boards put these genes on the same list. One is correct. Two are the wrong tumor suppressors. And one is the same gene pointing the wrong direction. Tap each card to flip.
No connection to the enteric nervous system or neural crest migration
Like TP53, this is a tumor suppressor. The disease is congenital neuronal absence, not a cancer.
The rule:Retinoblastoma gene + gut aganglionosis = zero overlap. Eliminate on sight.
Critical Contrast: RET is the only gene on this list that does both. RET LOSS-of-function = Hirschsprung (missing ganglion cells). RET GAIN-of-function = MEN2A/MEN2B and medullary thyroid carcinoma. Same chromosome 10, opposite direction, completely different disease. Boards love this contrast.
2 / 6
The Detective Trail
Work the Stem
Three clues. Three decisions. Make each call before the answer reveals. This is how boards think.
Step 1 of 3 · Read the Discriminator
A 2-day-old male neonate has not yet passed meconium. He is tachycardic and has bilious vomiting and a distended, tympanitic abdomen. A sweat chloride test returns 22 mmol/L. Abdominal X-ray shows dilated loops of bowel. The neonatologist orders a rectal suction biopsy.
The sweat chloride result of 22 mmol/L most effectively rules out which diagnosis?
Not Hirschsprung. Hirschsprung disease is a neurologic migration defect. Sweat chloride is a chloride transport test that has nothing to do with the enteric nervous system. A normal sweat chloride does not affect the likelihood of Hirschsprung.
Exactly right. Cystic fibrosis causes meconium ileus through CFTR-related chloride transport failure, producing thick, sticky meconium that plugs the ileum. The sweat chloride test directly measures CFTR function. A result of 22 mmol/L is well below the borderline range (40-59) and the diagnostic threshold (60+). CF is off the table. What remains is Hirschsprung.
Not intestinal atresia. Intestinal atresia is a structural defect, not a CFTR-mediated secretion defect. Sweat chloride has no diagnostic relationship to atresia.
Not anorectal malformation. Anorectal malformations are anatomic defects visible on physical exam. Sweat chloride does not bear on their diagnosis.
Step 2 of 3 · Interpret the Biopsy
The rectal suction biopsy is stained with H&E. The pathologist reports the finding that confirms Hirschsprung disease. Which finding was reported?
No ganglia at all, let alone hyperplastic ones. Hirschsprung disease is defined by absence of ganglion cells, not their overgrowth. Hyperplastic ganglia would actually suggest the opposite problem.
That is the diagnostic finding. Absence of ganglion cells in both the submucosal plexus (Meissner) and the myenteric plexus (Auerbach) is the pathognomonic finding of Hirschsprung disease on rectal suction biopsy. Without these cells, the distal segment cannot undergo coordinated relaxation and acts as a functional obstruction.
Neutrophilic infiltration suggests infection or ischemia, not Hirschsprung. Hirschsprung is a developmental neuronal deficiency, not an inflammatory process. Enterocolitis can complicate Hirschsprung, but the primary diagnostic finding is the absent ganglion cells.
Eosinophilic infiltration with crypt destruction is eosinophilic colitis or allergic colitis, not Hirschsprung. The defining lesion in Hirschsprung is neuronal, not inflammatory.
Step 3 of 3 · Name the Gene
The pediatric genetics service is consulted. They explain that the same gene that causes Hirschsprung disease, when it sustains a different type of mutation, causes MEN2A and medullary thyroid carcinoma. Which gene is this, and what type of mutation causes Hirschsprung?
RET gain-of-function is the MEN2 side, not the Hirschsprung side. You have the direction flipped. Activating RET = MEN2A/MEN2B = cancer. Loss of RET signaling = neural crest cells cannot migrate = Hirschsprung.
TP53 has no role in neural crest migration or the enteric nervous system. TP53 is a cell-cycle checkpoint protein that prevents malignant transformation. It does not guide embryonic migration.
Correct. RET (chromosome 10) is the gene. The loss-of-function side = Hirschsprung disease (neural crest cells fail to complete their migration to the distal bowel). The gain-of-function side = MEN2A and MEN2B, driving medullary thyroid carcinoma, pheochromocytoma, and parathyroid disease. Same gene, opposite mutation type, opposite disease. This is the boards contrast you must own.
CFTR is already excluded by the sweat chloride. CFTR also does not cause MEN2A or medullary thyroid carcinoma. This has nothing to do with RET.
3 / 6
Memory Hooks
Lock It In
Tap each card to reveal the hook. One read. It sticks.
Hook 1 · RET LOF vs GOF
How do you remember which direction of RET does what?
Think of RET as a light switch. Lose the switch (LOF): the neural crest cells have no guidance signal, they stop early, the distal bowel gets no ganglion cells = Hirschsprung. Flip the switch on permanently (GOF): the cells receive a constant activation signal, they become cancerous = MEN2 + medullary thyroid carcinoma. LOF = dark gut. GOF = cancer on fire. Same switch, same chromosome 10. Opposite direction. Opposite disease.
tap to reveal
Hook 2 · Sweat Chloride Cutoff
What does a sweat chloride of 22 mmol/L mean?
Three zones: Below 30 = normal (no CF). 30-59 = borderline (repeat and work up). 60 and above = diagnostic for CF. A result of 22 is stone-cold normal. It is as far from the CF threshold as you can get. When you see "sweat chloride 22" in a meconium-failure stem, your only job is to mentally cross out CFTR/CF/meconium-ileus and look for the real diagnosis. The test did exactly what it was designed to do: it killed CF. Now find the ganglion cells.
tap to reveal
Hook 3 · TP53 Kill
Why is TP53 such a compelling wrong answer here?
Because TP53 is the most famous tumor suppressor on the boards and you are primed to see it everywhere. But TP53 is the guardian of the genome: it guards against malignant transformation. A newborn with aganglionosis does not have cancer. The gut cells are completely normal except they have no neural support. TP53 governs whether cells become malignant when their DNA is damaged. It has zero role in whether an embryonic neural crest cell navigates the 25-centimeter journey from the neural tube to the rectum. Congenital aganglionosis = migration defect, not a cancer. TP53 is not invited to this diagnosis.
tap to reveal
Hook 4 · Squirt Sign
What is the squirt sign and why does it happen?
When the examiner performs a digital rectal exam in Hirschsprung disease, the finger enters the narrowed aganglionic segment. The moment it is withdrawn, stool rockets out. That is the squirt sign. Why does it happen? The aganglionic segment acts as a functional obstruction. Stool backs up under pressure in the ganglionic colon proximal to the blockage. When the finger temporarily opens the sphincter mechanism, the pressure differential drives explosive release. No squeeze needed from the infant. The obstructed pressure does all the work. If you see "explosive stool on withdrawal of rectal exam finger" in a neonate, you are reading a Hirschsprung stem.
tap to reveal
Hook 5 · Down Syndrome Association
Why is Hirschsprung disease more common in Down syndrome?
Trisomy 21 (Down syndrome) is the most common chromosomal association with Hirschsprung disease. About 2-10% of Hirschsprung patients have Down syndrome. The link is not perfectly understood but involves disrupted neural crest cell migration pathways that are also affected by trisomy 21 developmental effects. On boards: an infant with Down syndrome who fails to pass meconium should raise Hirschsprung immediately, even before a workup. Confirm with rectal suction biopsy (absent ganglion cells). Down syndrome + failure to pass meconium = think Hirschsprung first.
tap to reveal
4 / 6
Clinical Photos
What You Are Actually Seeing
Tap any image to enlarge. Recognize these findings on exam day.
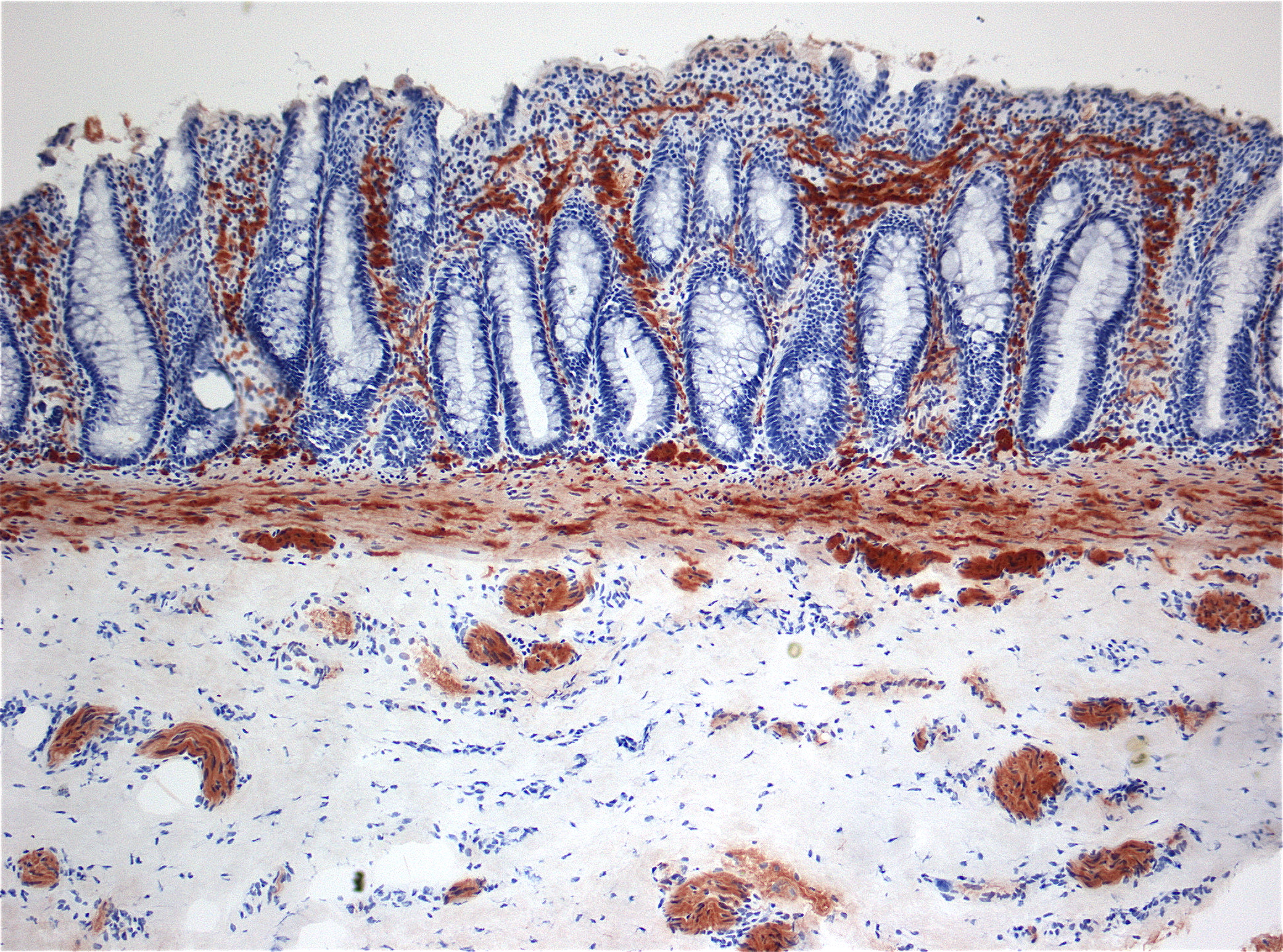
📷 Hirschsprung · Histopathology (AChE stain)
📷 Hirschsprung · Abdominal X-ray
📷 Hirschsprung · Chronic Colonic Distension
Hirschsprung Disease · HistopathologyAcetylcholinesterase (AChE) histochemistry demonstrating the aganglionic segment. Normal bowel has AChE-positive ganglion cells in Meissner and Auerbach plexuses. The Hirschsprung segment shows absent ganglion cells with hypertrophied nerve trunks. Rectal suction biopsy at 2 cm proximal to the dentate line is the standard diagnostic approach.Wikimedia Commons, public domain
Hirschsprung Disease · Abdominal X-rayDilated loops of bowel proximal to the aganglionic segment. The rectum and sigmoid may show absence of air (the functional obstruction zone). In the neonate: failure to pass meconium within 48 hours + proximal bowel distension = Hirschsprung until proven otherwise. Barium enema may show a "transition zone" between the narrow aganglionic segment and dilated proximal bowel.Wikimedia Commons, public domain
Hirschsprung Disease · Chronic Colonic Distension (Adult)Massively dilated colon (megacolon) from long-standing aganglionosis in an adult with delayed diagnosis. The dilated colon represents chronically obstructed stool proximal to the aganglionic zone. While most Hirschsprung presents in neonates or infants, short-segment disease may not be diagnosed until later. Boards test neonatal presentation most commonly.Wikimedia Commons, CC BY-SA 3.0
Biopsy Technique: Rectal suction biopsySuction biopsy is performed 2-3 cm above the dentate line in neonates. It samples the submucosa where Meissner plexus resides. The specimen is examined for presence or absence of ganglion cells. Full-thickness biopsy is the gold standard but suction biopsy is the standard first-line diagnostic tool. is the gold standard diagnostic test. The sample is taken 2-3 cm above the dentate line. Absence of ganglion cells in both the submucosal (Meissner) and myenteric (Auerbach) plexuses confirms Hirschsprung disease.
5 / 6
Board Walkthrough
Five Patients Just Walked In
Original board-style vignettes. Each one tests a different axis of this topic. No skipping.
The pattern is locked or it is not. Read the stem. Make the call. Tap the answer. Then work through every beat chain.
Board Vignette · 1 of 5
A 2-day-old male neonate has not yet passed meconium. He was born at 38 weeks gestation after an uncomplicated pregnancy. Physical exam reveals a distended abdomen with high-pitched bowel sounds. Bilious vomiting has occurred twice since birth. A sweat chloride test returns 22 mmol/L. Abdominal X-ray shows dilated bowel loops throughout. Rectal suction biopsy is performed and the pathology report reads: "No ganglion cells identified in the submucosal or myenteric plexus. Hypertrophied nerve trunks present."
Which genetic mutation is most responsible for this neonate's presentation?
ACFTR loss-of-functiontap to expand
Good instinct on connecting CFTR to meconium failure, because CF does cause meconium ileus. Think of it like a tollbooth on the chloride highway: when CFTR fails, the mucus thickens and the ileum gets a sticky plug. But here is the problem. The sweat chloride is 22 mmol/L. Normal is below 30. The diagnostic threshold for CF is 60. A result of 22 makes CFTR failure physiologically impossible in this context. Sweat chloride 22 = CFTR works fine = CF eliminated before you finish reading the stem.
BTP53 loss-of-functiontap to expand
TP53 is the most-tested tumor suppressor on the boards and you have been trained to look for it. But here is the mismatch: TP53 decides whether a cell with damaged DNA gets a chance to repair itself or gets sent to apoptosis. It is a goalkeeper for malignancy. This neonate has absent ganglion cells, which means neurons never arrived. That is a migration story, not a cancer story. TP53 protects against malignancy. Hirschsprung is congenital aganglionosis. These are categorically different problems.
CRET loss-of-functionCORRECT
The full package is here. Neonate, failure to pass meconium, bilious vomiting, abdominal distension, sweat chloride 22 (CF gone), biopsy showing absent ganglion cells with hypertrophied nerve trunks. This is Hirschsprung disease. The underlying cause is loss-of-function mutation in RET, the receptor tyrosine kinase that guides neural crest cell migration from the neural tube to the distal colon. Without functional RET signaling, those cells stop short and the distal segment stays aganglionic. RET LOF = failed neural crest migration = absent ganglion cells = Hirschsprung. Lock it.
DRB1 loss-of-functiontap to expand
RB1 encodes the retinoblastoma protein, the brake on the cell cycle at the G1/S checkpoint. When RB1 fails, the cell cycle runs unchecked and retinoblastoma develops in pediatric eyes. It also predisposes to osteosarcoma. There is no mechanism by which RB1 loss affects the enteric nervous system or neural crest cell migration. RB1 = eye tumor gene. Not a ganglion cell gene. Not for aganglionosis.
ERET gain-of-functiontap to expand
RET gain-of-function is actually in the right gene family, but it is the opposite direction and the opposite disease. An activating RET mutation constitutively fires the receptor, driving uncontrolled proliferation in neural-crest-derived C cells of the thyroid = medullary thyroid carcinoma in MEN2A/MEN2B. This baby does not have thyroid cancer. The RET switch is off (LOF), not stuck on (GOF). Same gene (chr 10), opposite mutation, completely different disease. Do not mix these up on boards.
Clue chain: neonate + no meconium at 48h + bilious vomiting + sweat chloride 22 (kills CF) + absent ganglion cells on biopsy = Hirschsprung disease. Gene = RET loss-of-function. The sweat chloride is the discriminator that arrives before the biopsy. Learn to kill CF in the first sentence.
Board Vignette · 2 of 5
A 3-week-old female infant is brought to the pediatrician for constipation since birth and progressive abdominal distension. She has passed only small amounts of stool, requiring rectal stimulation each time. On exam, the abdomen is distended and tympanitic. A sweat chloride test is performed and returns 22 mmol/L. The pediatrician explains that this result allows one diagnosis to be confidently excluded before ordering any further tests.
Which diagnosis does the sweat chloride result most effectively exclude?
AHirschsprung diseasetap to expand
Hirschsprung disease is a neurologic defect in the enteric nervous system. The sweat chloride test measures chloride transport function in exocrine glands. These two systems are completely unrelated. A normal sweat chloride tells you nothing about whether ganglion cells are present in the colon. Sweat chloride does not test the enteric nervous system. It cannot exclude Hirschsprung.
BIntestinal volvulustap to expand
Intestinal volvulus is a mechanical twisting of the bowel on its mesenteric axis, producing obstruction and ischemia. It is a structural diagnosis that requires imaging (upper GI series or CT showing the "whirlpool sign" of twisted mesentery). Sweat chloride does not diagnose or exclude mechanical bowel disease of any kind. Sweat chloride has zero relevance to volvulus.
CCystic fibrosis with meconium ileus equivalentCORRECT
The sweat chloride test was designed precisely to diagnose cystic fibrosis. CFTR loss-of-function impairs chloride secretion in all exocrine glands, including sweat glands. In CF, sweat chloride is elevated (above 60 mmol/L diagnostic, 40-59 borderline). A result of 22 is well below normal and makes CF physiologically impossible. This directly eliminates CFTR as the cause of this infant's constipation and obstruction. Meconium ileus (in neonates) and meconium ileus equivalent (in older CF patients) both require CF to be present. Without CF, these presentations cannot exist. Sweat chloride 22 = CFTR normal = no CF = no meconium ileus. Clean elimination.
DAnorectal malformationtap to expand
Anorectal malformations (imperforate anus, anal atresia, rectoperineal fistulas) are anatomic defects diagnosed by direct physical examination of the perineum at birth. They have no relationship to CFTR function or the sweat gland chloride transport system. A normal sweat chloride cannot exclude an anatomic defect. Anorectal malformations are physical exam findings. Sweat chloride is a biochemical test. They do not overlap.
The sweat chloride test has one job: determine if CFTR works. A result of 22 says it works normally. That instantly eliminates any diagnosis that requires CFTR failure (CF and its intestinal manifestations). Everything else on the differential still stands.
Board Vignette · 3 of 5
A genetics professor presents two cases at grand rounds. Case A: a neonate with failure to pass meconium, confirmed absent ganglion cells on biopsy, RET mutation found on sequencing. Case B: a 34-year-old woman with medullary thyroid carcinoma, bilateral pheochromocytomas, and hyperparathyroidism. Genetic testing also reveals a RET mutation on chromosome 10. The professor states that both patients share the same affected gene but carry fundamentally different mutation types.
Which pairing correctly describes the RET mutations in Case A and Case B?
ACase A = GOF; Case B = LOFtap to expand
You have the direction flipped. An activating RET (GOF) in an embryo would not cause aganglionosis. Neural crest cells use RET signaling to migrate. GOF would actually push cells to proliferate more, not stop short. The Hirschsprung phenotype requires loss of the migration signal (LOF). MEN2A requires a constitutively active signal (GOF). Hirschsprung = RET off (LOF). MEN2 = RET stuck on (GOF). You had them backwards.
BCase A = LOF; Case B = GOFCORRECT
Exactly right. Case A: RET loss-of-function. During embryogenesis, neural crest cells use RET receptor signaling to receive their "keep migrating" instruction from GDNF ligand. When RET fails (LOF), the cells lose their guidance system and stop short of the rectum. The result is an aganglionic distal segment = Hirschsprung. Case B: RET gain-of-function. An activating mutation locks RET in the "on" position in thyroid C cells, parafollicular cells, adrenal chromaffin cells, and parathyroid cells. The constitutive signaling drives malignant transformation = MEN2A (medullary thyroid carcinoma + pheochromocytoma + parathyroid hyperplasia). Same gene, chromosome 10, same name RET, opposite mutation direction, opposite disease consequence.
CBoth LOFtap to expand
If Case B (MEN2A) had a RET loss-of-function, there would be no constitutively active signal to drive C-cell proliferation. MEN2A requires an activating mutation. Loss-of-function RET in thyroid C cells would, if anything, impair their signaling. Medullary thyroid carcinoma in MEN2A depends on RET being stuck in the "on" position, not turned off. MEN2A requires RET gain-of-function. This is not negotiable.
DBoth GOFtap to expand
If Case A (Hirschsprung) had a RET gain-of-function, the neural crest cells would receive an amplified "go" signal and, if anything, would over-migrate or over-proliferate. Hirschsprung disease results from absent migration signal (RET is non-functional). The aganglionic segment cannot be explained by an overactive RET. Hirschsprung requires RET loss-of-function. The cells needed RET to work; it did not.
The RET contrast is the boards' favorite genetics question on Hirschsprung. Know it forward and backward. LOF = Hirschsprung (migration fails, gut loses its nerve). GOF = MEN2A/MEN2B (cells gain uncontrolled proliferative drive, cancer develops in RET-expressing lineages).
Board Vignette · 4 of 5
A surgical pathologist receives a rectal suction biopsy specimen from a 3-day-old male with failure to pass meconium and abdominal distension. The referring neonatologist has documented a sweat chloride of 28 mmol/L. The biopsy is taken 2 cm above the dentate line. On H&E staining, the pathologist examines the submucosa and muscularis propria carefully. The final report will either confirm or exclude the presumed clinical diagnosis.
Which of the following biopsy findings would confirm the most likely diagnosis in this infant?
AHyperplastic ganglia with mitosestap to expand
Good instinct if you thought "neuronal problem = something wrong with neurons." But the direction is wrong. Hirschsprung disease is defined by neuronal absence, not neuronal overgrowth. There are no ganglion cells to be hyperplastic. What is actually found are hypertrophied nerve trunks (cholinergic fibers without ganglion cell bodies), which helps explain the constipation by a different mechanism. Hirschsprung = no ganglion cells at all. Cannot hyperplasia what does not exist.
BDense eosinophilic infiltration of the lamina propriatap to expand
Eosinophilic colitis is an immune-mediated or allergic inflammatory condition. It has characteristic eosinophils filling the lamina propria and sometimes forming sheets around crypts. This is entirely unrelated to the enteric nervous system defect in Hirschsprung disease. The clinical picture (failure to pass meconium in a neonate, not an allergic presentation) does not fit eosinophilic colitis. Eosinophilic infiltration = allergic/immune. Not the neural defect of aganglionosis.
CAbsent ganglion cells in both plexusesCORRECT
This is the pathognomonic finding of Hirschsprung disease. The rectal suction biopsy samples the submucosa, where Meissner plexus resides, and ideally includes a piece of the muscularis propria where Auerbach plexus lies. Both must be absent for a definitive diagnosis. The sweat chloride of 28 already killed CF. The biopsy seals the diagnosis. This is the finding that takes a clinical suspicion and converts it into a confirmed diagnosis requiring surgical intervention (pull-through procedure to remove the aganglionic segment). Absent ganglion cells in Meissner + Auerbach plexuses = Hirschsprung confirmed. This is the pathology report you want to see.
DGranulomatous inflammation surrounding intact gangliatap to expand
Granulomatous inflammation in the bowel wall with intact ganglia would suggest Crohn disease (granulomatous colitis) or potentially a fungal/mycobacterial infection. Crohn disease is not a neonatal presentation, does not cause failure to pass meconium at birth, and does not involve the enteric nervous system. Also, Hirschsprung does not show inflammation around ganglia because there are no ganglia to surround. Granulomas = Crohn or infectious. Not Hirschsprung. Fundamentally wrong tissue findings.
ETransmural neutrophilic infiltration with crypt abscessestap to expand
Transmural neutrophilic infiltration with crypt abscesses is the histology of ulcerative colitis or severe infectious colitis. Ulcerative colitis does not present in neonates and is characteristically a mucosal disease without transmural involvement. This is not a picture that fits congenital aganglionosis. The clinical context alone (3-day-old neonate, meconium failure) should eliminate colitis from consideration before you even get to the biopsy result. Crypt abscesses = colitis (UC or infectious). Not the congenital neuronal defect of Hirschsprung.
The diagnostic triad: (1) neonate with failure to pass meconium in 48 hours, (2) normal sweat chloride excluding CF, (3) rectal suction biopsy showing absent ganglion cells in Meissner and Auerbach plexuses. All three together close the diagnosis and open the surgical plan.
Board Vignette · 5 of 5
A newborn male with trisomy 21 (Down syndrome) is evaluated by the neonatology team on day 2 of life. He has not passed meconium. On physical exam, his abdomen is distended. Digital rectal examination is performed; upon withdrawal of the examining finger, there is explosive expulsion of stool and gas. A sweat chloride is ordered and returns 19 mmol/L. Rectal suction biopsy confirms the diagnosis.
Which mutation is most likely responsible for this infant's intestinal pathology?
ACFTR loss-of-functiontap to expand
This is the most predictable wrong answer on Hirschsprung questions and the boards know it. The sweat chloride of 19 mmol/L is stone-cold normal. Normal is below 30. The diagnostic threshold for CF is 60. A result of 19 is as far from a CF diagnosis as you can be. CFTR is definitively off the table before you have even considered the other clues. Sweat chloride 19 = CFTR intact = CF impossible. Move on immediately.
BTP53 loss-of-functiontap to expand
TP53 is a genome guardian. It prevents cancer. This newborn's problem is that his neurons never arrived to his distal colon. TP53 is not involved in embryonic neural crest cell migration, GDNF signaling, RET receptor function, or enteric nervous system development. Think of it like this: you would not call a cancer immunologist to fix a plumbing problem in a house under construction. The systems do not overlap. TP53 = malignancy checkpoint. Hirschsprung = missed migration deadline. Different departments entirely.
CRB1 loss-of-functiontap to expand
RB1 is the cell-cycle brake at the G1/S checkpoint. Its loss leads to retinoblastoma in pediatric eyes and predisposes to osteosarcoma. There is no RB1 connection to the enteric nervous system or to trisomy 21 intestinal complications. RB1 is on chromosome 13. Hirschsprung is driven by RET on chromosome 10. These are completely different genetic pathways. RB1 = retinoblastoma. Eye. Cell cycle. Not the gut. Not migration.
DRET loss-of-functionCORRECT
All clues converge here. Down syndrome is the most common chromosomal association with Hirschsprung disease. The explosive stool on withdrawal of the rectal exam finger is the classic squirt sign, caused by stool backed up under pressure behind the aganglionic zone. The sweat chloride of 19 eliminates CF. The biopsy confirmed absent ganglion cells. Underlying cause: RET loss-of-function, which disrupted neural crest cell migration during weeks 5-12 of gestation. The aganglionic segment acts as a functional obstruction that cannot spontaneously relax. Trisomy 21 + no meconium + squirt sign + normal sweat chloride + absent ganglion cells = Hirschsprung = RET loss-of-function.
EBRCA1 loss-of-functiontap to expand
BRCA1 is a DNA-repair gene involved in homologous recombination. Its loss-of-function predisposes to hereditary breast and ovarian cancer in adults. It has absolutely no role in embryonic neural crest cell migration, enteric nervous system development, or neonatal bowel obstruction. Why is it here? To make sure you are not just pattern-matching on "loss-of-function" without knowing what each gene actually does. BRCA1 = adult breast/ovarian cancer predisposition. Not a neonatal GI migration gene. Eliminate without hesitation.