The biggest branch of the femoral artery, and the most seductive wrong answer in the femoral-head blood-supply question. It feeds the whole thigh. It does not feed the head. Its little branch does.
Quick Challenge
A 7-year-old boy has 8 weeks of insidious left thigh pain and a limp, no trauma. Abduction and internal rotation are restricted, the leg rests in external rotation, and the hip forces into external rotation on flexion. Pelvic radiograph shows widening of the left hip joint. Idiopathic avascular necrosis of the femoral head is diagnosed. Interruption of which artery best explains the dead bone?
This is Legg-Calve-Perthes, idiopathic avascular necrosis of the femoral head in a child. The head lives on the medial circumflex femoral artery and its retinacular branches climbing the posterior neck. The deep femoral is the trap: it is the parent of the medial circumflex, one step too far upstream. Cut the deep femoral trunk and the whole thigh would starve, not one selective spot on the head. Scroll down and watch exactly why the big artery loses to its own little branch.
↓ scroll to dismantle the trap
Section 1 · Know the vessel
Meet the Profunda
Before you can call it a wrong answer, you have to know it cold. The deep femoral is a real, important, frequently-bleeding artery. Tap through its four facets.
Where it starts
Origin and Course
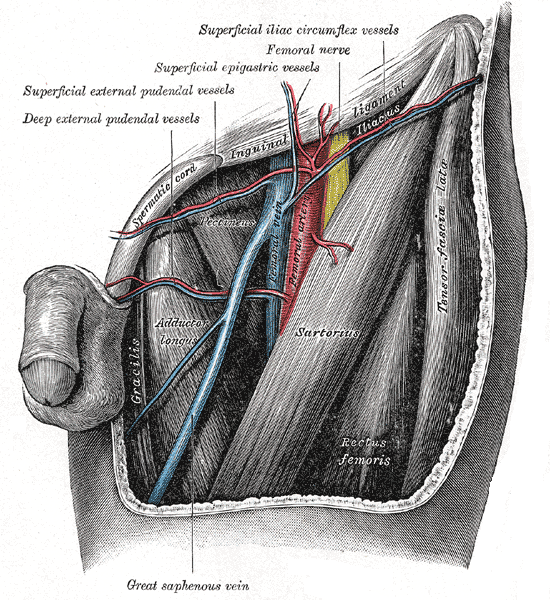
The deep femoral is the largest branch of the femoral artery. It comes off the posterolateral side of the femoral artery in the femoral triangleThe hollow just below the groin crease, bounded by the inguinal ligament, sartorius, and adductor longus. The femoral artery, vein, and nerve run through it, so any vessel here is surgically and clinically exposed., about 3.5 cm below the inguinal ligament.
The split that matters
At that branch point the femoral artery effectively divides into two roles: the superficial femoral continues down to the knee (becomes the popliteal), and the deep femoral dives backward to run the thigh. Same parent, two completely different jobs.
Why "3.5 cm" is a clue
That short distance is exactly why a stab or a catheter low in the femoral triangle can hit the deep femoral instead of the main trunk. Location is the whole story in vascular questions.
The femoral triangle, just below the groin. The deep femoral peels off here, about a finger-width down.
Profunda means "deep." It dives DEEP and BACK to run the thigh, while the superficial femoral stays the highway to the knee. Deep femoral = deep thigh, not the head.
What comes off it
The Branches
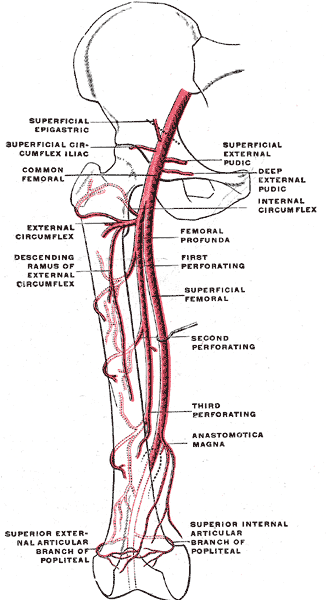
The deep femoral is a parent vessel. Its named children are the two circumflex arteries and the perforators.
Medial circumflex femoral (MCFA)
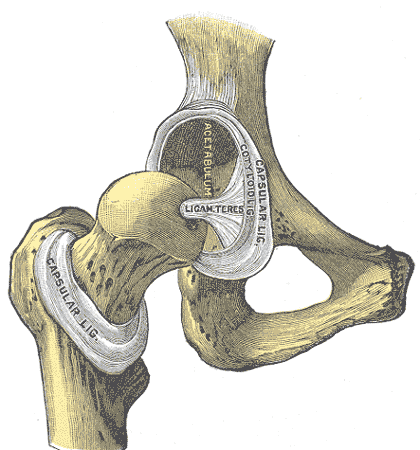
Wraps the posterior femoral neck and sends retinacular arteriesTiny vessels that run UP the femoral neck inside folds of the joint capsule (the retinacula). They are the actual pipes delivering blood to the head, which is why a neck fracture that tears them starves the head. up to the head. This is the branch the femoral head lives on.🔑Medial Circumflex = Main Circulation to the head. The M words travel together.
Lateral circumflex femoral (LCFA)
Runs laterally behind sartorius and rectus femoris, supplies the anterolateral thigh and contributes to the cruciate and trochanteric anastomoses. Minor player in head supply.
3 to 4 perforating arteries
They pierce the adductor magnus to reach the posterior thigh. These are the real workhorses feeding the thigh muscles.🔑Perforators Pierce. They punch through adductor magnus to reach the back of the thigh. Picture them drilling holes.
One trunk, three jobs. The deep femoral hands off the two circumflex arteries and the perforators.
One trunk, three jobs: medial circumflex (to the head), lateral circumflex (to the side), perforators (to the muscle). Only the medial circumflex matters for avascular necrosis.
What it actually feeds
Territory
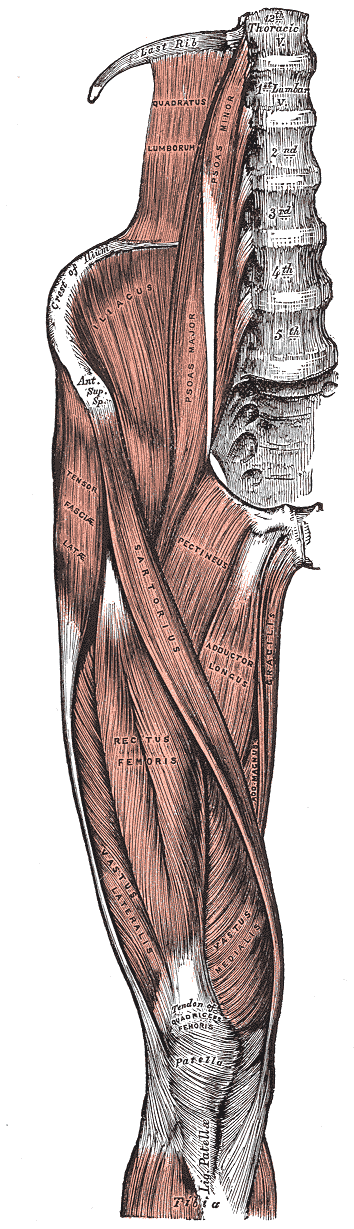
This is the part the trap depends on you forgetting. The deep femoral is the main blood supply to the thigh musculature: the adductors, the hamstrings, and the vastus group of the quadriceps.
How it reaches them
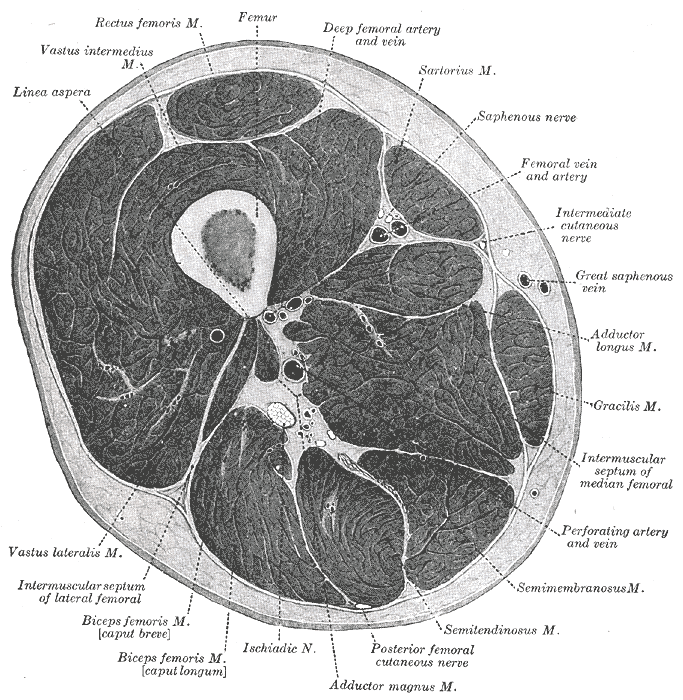
Through the perforating arteries that pierce adductor magnus and fan out to the posterior and medial compartments. The cross-section plate below labels exactly this.
A slice through the thigh. The perforators punch back through the muscle to feed every compartment.
The logical consequence
If you sacrifice the whole deep femoral trunk, you do not get a tidy little patch of dead bone on the femoral head. You get a thigh in trouble: widespread muscle ischemia. That mismatch is the kill shot against this distractor.
The muscle country it powers: adductors, quads, and the hamstrings behind them.
The deep femoral is the thigh's power company. Avascular necrosis of the head is a single-bulb outage. You do not blame the whole power company for one dead bulb fed by one small wire.
Where it shows up in real medicine
Clinical
The deep femoral has its own real exam appearances. It is a wrong answer for the femoral head, but a right answer elsewhere.
Penetrating thigh bleeds
Deep posterior thigh stab wounds and pseudoaneurysms classically involve the deep femoral or its perforators, because they sit deep against the bone where pressure is hard to apply.
Collateral rescue
When the superficial femoral artery slowly occludes (classic in peripheral artery disease), the deep femoral perforators become the detour that keeps the lower leg alive. The limb survives on the artery the boards keep calling the distractor.
Cruciate anastomosis
A cross-shaped junction behind the proximal femur formed by the MCFA + LCFA (both from the deep femoral), the inferior gluteal, and the first perforating artery. It links the gluteal and femoral circulations.🔑Cruciate = a CROSS. Four roads meet: two circumflex (medial + lateral), inferior gluteal from above, first perforator from below.
Deep femoral facts that are TRUE: it bleeds in deep thigh trauma, it rescues the leg in superficial femoral occlusion, and it builds the cruciate anastomosis. None of those is "feeds the femoral head."
Section 2 · The mechanism
The Head's Real Lifeline
Watch the blood actually travel. One press runs the whole sequence: trunk, to branch, to the retinacular vessels, to the head. See exactly where the deep femoral hands off.
The head the trap cannot reach. It feeds off the medial circumflex retinacular vessels, not the big trunk.
The patient on the table
THEO
Age 7 · 8 weeks of limp
"His left hip just stopped moving right. No fall, no fever. The head of his femur is dying. Find the pipe that feeds it."
The deep femoral trunk pulses. Watch where it hands off.
ONE STEP TOO PROXIMAL
Route
Deep femoral → medial circumflex femoral → retinacular arteries → head
Pattern
Head infarct = the retinacular branch is cut, not the trunk
Pearl
Cut the trunk and the whole thigh dies. Cut the branch and only the head dies. Boards want the branch.
The deep femoral is the address one block too far up the street. The medial circumflex is the door the blood actually walks through.
Section 3 · The board set
The 5-Artery Showdown
This is the actual question: five arteries, one feeds the femoral head. Each clue kills one impostor. Tap the artery the clue eliminates. Last one standing is your answer.
Eliminate the impostors
Loading clue...
Inferior gluteal artery
Superior gluteal artery
Artery of ligamentum teres
Deep femoral artery
Medial circumflex femoral
The Chicago breakdown, all five at once:
Inferior gluteal: buttock and the companion artery of the sciatic nerve. It hurts in the glutes, not the hip joint. No retinacular vessels to the head. Wrong neighborhood.
Superior gluteal: powers the hip abductors. Knock it (or its nerve) out and the pelvis drops on the opposite side, a waddling TrendelenburgWhen the abductors (gluteus medius and minimus) fail, the pelvis sags toward the unsupported side during single-leg stance, producing a lurching gait. It is an abductor problem, not a blood-supply-to-the-head problem. gait. The head still gets blood. Wrong job.
Artery of ligamentum teres: a tiny twig in the round ligament. It matters in a toddler, then fades. In a 7-year-old it is already a bit player, far too small to be the main supply. Too small.
Deep femoral: the big trunk that feeds the WHOLE thigh. Cut it and the entire thigh starves, not one selective spot on the head. One branch too far upstream. The trap.
Medial circumflex femoral: wraps the posterior femoral neck, sends retinacular arteries up to the head. THIS is the lifeline. Interrupt it and you get avascular necrosis. The answer.
Section 4 · The reasoning move
Walk the Logic
Three forks. Guess before each reveal. This is the exact chain that takes you from "dead femoral head" to the single right vessel without falling for the trunk.
Fork 1: A femoral head is dying. Is the problem a big regional supply or a small dedicated pipe?
Either tap teaches the same lesson: a selective head infarct points to a small dedicated vessel. If a big regional trunk failed, you would see widespread muscle ischemia too, not an isolated dead head. So you are hunting a small artery that goes specifically to the head.
Fork 2: Which small vessel carries the bulk of that supply in a child or adult, past infancy?
The retinacular branches of the medial circumflex femoral carry the bulk. The ligamentum teres artery is a real vessel, but its contribution is large only in early childhood and shrinks with age. Past infancy the head leans on the medial circumflex. So your vessel is the medial circumflex femoral.
Fork 3: The deep femoral is the parent of that medial circumflex. Why is the deep femoral still wrong?
It is one step too proximal. The deep femoral does connect to the head, through its medial circumflex branch, but the trunk also feeds the entire thigh musculature. The question asks for the vessel whose loss explains a selective head infarct, and that is the branch, not the trunk. Name the branch: medial circumflex femoral. Done.
Section 5 · Board reps
Clinical Walkthrough
Original board-style vignettes. Answers shuffle each round. Right-click or long-press to cross out options. Double-tap to highlight.
VIGNETTE 1 OF 6
Section 6 · Lightning round
Rapid Quiz
Five questions pulled from a bigger pool, reshuffled every load. Do not overthink the trunk-versus-branch ones.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.