A narrowed renal artery fools the kidney into thinking the whole body is underperfused, so it makes pressure. Two very different patients cause that narrowing, and the board reward is telling them apart and tracing the cascade they trigger.
The miss this page fixes: a student saw resistant hypertension, low potassium, and a high aldosterone and called it Conn primary hyperaldosteronism. But the renin was high, not suppressed, and the angiogram showed beading. High aldosterone is not automatically Conn. Check the renin first.
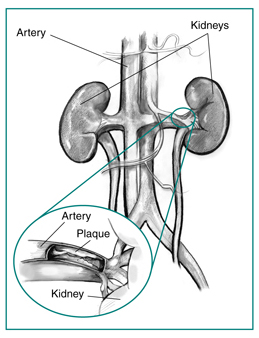
A 33-year-old woman has headaches and blood pressure that stays high despite three medications. On examination there is an abdominal bruit. Potassium is 3.3 mEq/L; plasma renin and aldosterone are both elevated. A renal angiogram shows a string of beads in the distal renal artery.
High renin AND high aldosterone is the renovascular pattern: the narrowed kidney is screaming for pressure, so it drives renin, which drives aldosterone. Conn syndrome also has a high aldosterone, but the renin is switched OFF, because the adrenal makes aldosterone on its own.
The young woman, the abdominal bruit, and the string of beads in the distal artery name the cause: fibromuscular dysplasia. Atherosclerotic stenosis is the older smoker with a proximal, ostial plaque, and essential hypertension has no focal beading or bruit. High renin plus high aldosterone equals renovascular, and beading in a young woman equals fibromuscular dysplasia.
Quick route: what is renal artery stenosis actually doing to the body?
Right. The narrowing is local, but the kidney reads it as whole-body hypotension and turns on renin, angiotensin, and aldosterone. That cascade is the disease.
The Frame
A narrowed renal artery makes the kidney scream for pressure
One cascade runs through this whole page. The kidney cannot tell a pinched renal artery from a bleeding-out body. It reacts the only way it knows: turn on the renin-angiotensin-aldosterone system. Learn the cascade once and the lab patterns and drug traps fall out of it.
🟫 The lesion narrows the artery
A stenosis, whether a string-of-beads dysplastic lesion or an ostial plaque, drops blood flow into that kidney. Perfusion pressure beyond the narrowing falls.
The kidney downstream now sits in a low-pressure pocket the rest of the body does not feel.
🔬 The juxtaglomerular apparatus senses it
The JGA reads the low flow as low systemic pressure and releases renin. Renin converts angiotensinogen to angiotensin I, and ACE makes angiotensin II.
The affected kidney pours out renin; the normal kidney suppresses its own. That asymmetry is diagnostic.
⚡ Angiotensin II and aldosterone amplify
Angiotensin II constricts vessels, and it clamps the efferent arteriole hardest to defend the glomerular filtration pressure. Aldosterone rises and retains sodium and water.
Remember the efferent squeeze: it is what an ACE inhibitor later removes.
📈 Renovascular hypertension
Vasoconstriction plus salt and water retention drive the blood pressure up. The chronically starved kidney atrophies and shrinks, which is why unilateral disease gives asymmetric kidney sizes.
The whole syndrome is renin-driven secondary hypertension.
The lab signature to lock in
Renovascular hypertension is secondary hyperaldosteronism: high renin AND high aldosterone, usually with a hypokalemic metabolic alkalosis and a high-normal sodium. Contrast Conn primary hyperaldosteronism: high aldosterone but low (suppressed) renin, because the adrenal makes aldosterone on its own. High renin plus high aldosterone equals the kidney is screaming for pressure.
🟫 Renal arteries branch off the abdominal aorta
The renal arteries arise from the abdominal aorta. The ostium (origin at the aorta) is where atherosclerotic plaque sits; the distal artery is where dysplastic beading appears. Tap to expand.
Tap each line to reveal the mechanism.
Why does the kidney raise the whole body's pressure when only its own artery is narrowed?
The juxtaglomerular apparatus cannot tell a local stenosis from real, whole-body hypotension. It senses low flow at its doorstep and reacts as if the entire circulation is failing, so it turns on renin. A local plumbing problem gets answered with a system-wide pressure response.
Why does angiotensin II clamp the efferent arteriole specifically?
The efferent arteriole is the drain on the far side of the glomerulus. Squeezing the drain raises the pressure inside the glomerular capillaries and props up the filtration rate even though inflow is poor. The efferent squeeze is the kidney's way of defending GFR, and it is exactly what an ACE inhibitor removes.
Why is the affected kidney small with a lopsided renin?
Chronic low perfusion starves and shrinks the affected kidney while it keeps pumping out renin. The healthy kidney, seeing the high pressure, shuts its own renin off. Asymmetric kidney sizes plus high renin on the affected side point straight at unilateral renal artery stenosis.
Two Causes
Same narrowing, two completely different patients
Tap between them. The cascade is identical, but the demographics, the wall layer, the lesion location, and the treatment all split cleanly. That split is what board questions test.
Fibromuscular Dysplasia
Atherosclerotic RAS
Fibromuscular Dysplasia
Young to middle-aged woman, distal artery, string of beads.
Who gets it
Young to middle-aged women. The leading cause of renal artery stenosis in this group. No relationship to smoking or cholesterol.
Treatment
Percutaneous transluminal balloon angioplasty (PTA), frequently curative or markedly improves the blood pressure, especially with short hypertension duration. A stent is generally not required.
The wall layer
Non-inflammatory, non-atherosclerotic thickening of the arterial wall. Tunica media proliferation (medial fibroplasia is the most common subtype).
Where the lesion sits
Distal two-thirds of the renal artery or its segmental branches, away from the aortic origin.
📸 String of beads (renal FMD)
The hallmark: alternating stenoses and small aneurysmal dilations give a string-of-beads look on angiography. Tap to expand.
Hallmark sign
String of beads on angiography: alternating areas of narrowing and small aneurysmal dilation.
Other arteries it loves
The internal carotid arteries: headache, pulsatile tinnitus, transient ischemic attack, and a risk of dissection.
🧠 String of beads (carotid FMD)
FMD is a systemic arteriopathy. The same beading appears in the internal carotid, explaining headache, pulsatile tinnitus, and dissection. Tap to expand.
Board Trap
The high-yield treatment answer is balloon angioplasty, often curative. Some review sources write it as angioplasty with or without stenting, but routine stenting is not the answer and FMD is not incurable. Do not jump to lifelong drug therapy and miss a fixable lesion.
Older patients, classically male smokers with coronary artery disease, claudication, or other atherosclerosis. The most common cause of renal artery stenosis overall (about 90 percent).
Treatment
Optimal medical therapy first: blood pressure control, a statin, aspirin, and smoking cessation. Revascularization is selective, not routine.
The wall lesion
Atherosclerotic plaque, the same disease that clogs coronaries and carotids, deposited in the renal artery.
Where the lesion sits
Proximal one-third, ostial (right at the aortic origin), often as a spillover plaque from the aorta itself.
🟫 Proximal ostial plaque (illustration)
Illustration of a proximal, ostial atherosclerotic plaque narrowing the renal artery near its aortic origin. Tap to expand.
The dangerous presentations
Resistant hypertension after about 55, an abdominal bruit, and flash pulmonary edema with refractory hypertension when disease is bilateral.
The drug clue
An acute rise in creatinine after starting an ACE inhibitor or ARB points to bilateral atherosclerotic disease.
Board Trap
The triad of severe or resistant hypertension, an abdominal bruit, and flash pulmonary edema should make you think bilateral atherosclerotic renal artery stenosis. Watch the creatinine and potassium if you start a RAAS blocker.
Two Patients, One Narrowing
Sort each clue into the patient it belongs to
No timer. A clue appears. Decide whether it fits the dysplastic young woman or the atherosclerotic older smoker. Each clue explains itself so the pattern locks in.
Fibromuscular Dysplasia
Young woman · distal artery · beads
Atherosclerotic RAS
Older smoker · proximal ostial · plaque
Tap a clue below to begin.
The Engine Room
Watch the cascade fire, then add the ACE inhibitor
Step through the renin cascade one beat at a time. The payoff is the last beat: when you add an ACE inhibitor in bilateral disease, the efferent squeeze that was propping up filtration is released, and you feel the trap.
The Glomerulus · Renovascular Lab
THE NARROWED ARTERY
Renal artery stenosis · either cause
"Flow into this kidney is choked off. Trace what the kidney does about it, beat by beat, then we will add a RAAS blocker and watch the filter."
The cascade is firing
Step 1. The renal artery is narrowed, so flow into this kidney falls.
NarrowingJGA · ReninAng II · AldoHypertension
Now add an ACE inhibitor in bilateral disease. What happens to the creatinine?
DefenseAngiotensin II clamps the efferent arteriole to hold up the filtration pressure
TrapAn ACE inhibitor or ARB removes the efferent squeeze, GFR falls, and creatinine rises: the bilateral renal artery stenosis trap
⚡ The renin-angiotensin-aldosterone system
The full RAAS pathway: low renal perfusion drives renin, then angiotensin II and aldosterone, raising blood pressure and retaining sodium. Tap to expand.
Bedside to Diagnosis
The clues that say stenosis, and the tests that prove it
Renal artery stenosis hides inside a hypertension workup. Three clusters of clues flag it, then a clean diagnostic ladder confirms it. Commit to a first test before the ladder opens.
🔎 When to suspect it
Resistant hypertension (uncontrolled on three or more drugs) or new severe hypertension, with onset before about 30 (young woman points to dysplasia) or after about 55 (older smoker points to atherosclerosis). Listen for an abdominal or flank bruit, and look for asymmetric kidney sizes.
Asymmetric kidney size means unilateral disease: the starved kidney shrinks.
💊 The medication clue
An acute rise in creatinine of more than about 30 percent after starting an ACE inhibitor or ARB is the classic clue to bilateral renal artery stenosis. You removed the angiotensin II that was holding up filtration.
Monitor creatinine and potassium whenever you start a RAAS blocker in suspected stenosis.
🌊 The dangerous triad
Flash pulmonary edema with refractory hypertension and an abdominal bruit should make you think bilateral renal artery stenosis. The sudden volume cannot escape a stiff, pressure-locked circulation.
Severe or resistant hypertension plus bruit plus flash pulmonary edema is the bilateral-disease triad.
You suspect renovascular hypertension in a patient with resistant blood pressure and an abdominal bruit. Renal function is currently stable.
Before the ladder opens: what is the best INITIAL test to screen for it?
1. Screen: renal duplex ultrasonography, noninvasive, shows the narrowing, elevated velocities, and asymmetric kidney sizes.
2. Confirm noninvasively:CT angiography or MR angiography (MRA is a strong answer for dysplasia, avoiding contrast load).
3. Gold standard:catheter renal arteriography shows the string of beads and lets you balloon the lesion in the same sitting.
Why not the others: biopsy is not how you diagnose stenosis, urine metanephrines chase pheochromocytoma, and the aldosterone-to-renin ratio chases primary hyperaldosteronism.
🧬 CT angiography (renal FMD)
CT angiography of renal-artery fibromuscular dysplasia. Cross-sectional angiography confirms the lesion noninvasively before catheter arteriography. Tap to expand.
Tap each line for the reasoning and the treatment.
Why start with a duplex ultrasound instead of jumping to angiography?
It is noninvasive, uses no contrast, and screens well: it shows the narrowing, the high flow velocities across it, and the asymmetric kidney sizes. You escalate to CT or MR angiography, and finally catheter arteriography, only as you need more detail or treatment. Screen noninvasively first, save the catheter for confirmation and therapy.
What does catheter arteriography add beyond confirming the diagnosis?
It is the gold standard for showing the string of beads, and it is also therapeutic: the interventionalist can perform balloon angioplasty in the same session. The gold-standard test for dysplasia can fix the lesion at the same time.
So how is each cause treated?
Dysplasia: percutaneous transluminal balloon angioplasty, frequently curative, stent not routine. Atherosclerotic: optimal medical therapy first (blood pressure control, statin, aspirin, smoking cessation) with selective revascularization. An ACE inhibitor or ARB is first-line for renovascular hypertension in unilateral disease (monitor creatinine and potassium) but is used with caution or avoided in bilateral disease because of the acute kidney injury risk.
One sentence to carry into the exam
Young woman plus beads plus high renin equals dysplasia; older smoker plus ostial plaque equals atherosclerosis; a creatinine jump after a RAAS blocker equals bilateral disease.
First, decide
The crashing patient: pick the FIRST move before the branch opens
Challenge yourself before the algorithm shows. Commit to a first move, then see the full branch.
A patient on the monitor has a potassium of 7.2 mEq/L with widening QRS complexes on the screen. You have calcium, insulin and glucose, albuterol, and a dialysis nurse on the way.
Before you see the algorithm: what is your FIRST move?
1. STABILIZE. ECG changing? IV calcium gluconate now. Minutes to act, protects the heart, buys you the rest of the sequence.
2. SHIFT. Insulin + glucose (workhorse), nebulized albuterol. Bicarbonate only if acidotic. Buys 30 to 60 minutes.
3. ELIMINATE. Loop diuretic if making urine, potassium binders, and dialysis (definitive in renal failure).
Memory peg: 4.5 is the bouncer for pH; for potassium the peg is "calcium clears the door first." Protection before everything.
Make it stick
Five hooks for the order and speed traps
Tap each card to reveal the hook. These are built to survive a tired night before the exam.
💚
Hyperkalemia order
Stabilize, shift, eliminate. Calcium first keeps the heart beating. It does not lower the number. Protect, then move it, then remove it.
tap to reveal
📋
List vs order
A drug list is not a drug order. Calcium goes in first no matter where it lands in the acronym. Letter order is not clinical order.
tap to reveal
🧬
Sodium speed
Sodium both ways, go slow. Too fast UP gives demyelination. Too fast DOWN gives brain swelling. The speed is the emergency, not the number.
tap to reveal
🧮
Magnesium unlock
You cannot fix potassium or calcium until you fix the magnesium. The quiet electrolyte controls the loud ones.
tap to reveal
🩸
Mag toxicity
Lost reflexes on a mag drip equals magnesium toxicity. Reach for calcium gluconate, stop the drip, protect the airway. Classic in preeclampsia.
tap to reveal
Board Walkthrough
The full clinical bank
teaching vignettes. One at a time, shuffled, never repeats until the bank is exhausted. Right-click or long-press a choice to cross it out. Double-click or double-tap to highlight.
Vignette 1 of 8
Sources: Built from standard board-review physiology and emergency management of fluid and electrolyte disorders. Membrane-stabilization, transcellular shift, and elimination logic per general internal medicine and critical care references. All vignettes are original and rebuilt from mechanism.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.