Same narrowed artery, opposite treatment. The right move depends on why the vessel narrowed and on the patient in front of you. The board traps are reflex stenting, lifelong pills for a curable lesion, and the creatinine that climbs the week you start an ACE inhibitor.
The miss this page kills: a learner saw a renal artery narrowing on imaging and reached for a stent, because fixing the picture felt like fixing the patient. A narrowing on a scan is not, by itself, a reason to revascularize. The cause and the clinical picture decide the treatment, not the image.
A 34-year-old woman has hypertension that stays high despite three drugs. She does not smoke. Renal angiography shows a beaded, "string of beads" segment in the distal right renal artery. Her creatinine is normal.
What is the best next step to control her blood pressure?
Place a renal artery stent across the narrowing
Percutaneous balloon angioplasty, without a stent
Commit her to lifelong ACE inhibitor therapy and accept the pressure
Proceed straight to aortorenal bypass surgery
Balloon angioplasty. The string of beads is fibromuscular dysplasia, and you can cure the pressure.
A young woman with resistant hypertension and a beaded distal artery has fibromuscular dysplasia. The move is percutaneous balloon angioplasty, and it is frequently curative of the hypertension, especially treated early. No stent goes in unless a complication like a dissection forces it.
Stenting is the atherosclerotic-ostium move, not the FMD move. An ACE inhibitor would control her pressure but settles for management when a cure is on the table. Surgery is the bailout for complex or failed cases. FMD: balloon the pipe, and you may fix the blood pressure for good.
Quick route: which single fact decides the treatment of renal artery stenosis the most?
Right. The cause drives the management. The percent narrowing alone does not tell you whether to balloon, stent, give meds, or leave it alone.
The Frame
Same narrowing, opposite management. Ask why it narrowed.
One question runs through every renal artery stenosis decision: what caused the narrowing, and what is the patient doing right now? Answer that and the treatment falls out.
🧶 FMD: fix the pipe
Young to middle-aged woman, a beaded "string of beads" in the distal two-thirds of the artery. The move is balloon angioplasty (PTA), no routine stent, and it is frequently curative of the hypertension. Medication controls the pressure, but angioplasty can cure it.
Best results when treated early and the hypertension is short-lived.
🥩 Atherosclerosis: treat the patient
Older patient, often a smoker, a proximal or ostial plaque. First-line is optimal medical therapy: an ACE inhibitor or ARB plus a statin, aspirin, smoking cessation, and risk-factor control. Routine stenting adds no benefit. Revascularize only for specific indications.
Large randomized trials settled that a stenosis alone is not a reason to stent.
💊 Untreated pressure: start the right drug
For renovascular hypertension, an ACE inhibitor or ARB is first-line. Unilateral disease: safe, just monitor.Bilateral disease (or a solitary kidney): watch the creatinine closely, because filtration there depends on angiotensin II.
Check creatinine and potassium one to two weeks after starting.
The one sentence to carry in
The cause and the clinical picture choose the treatment, not the image. Balloon the fibromuscular pipe, treat the atherosclerotic patient with medicine, and stent only when a real indication forces your hand. A narrowing on a scan is never, by itself, the reason to revascularize.
Tap each line to reveal why the routing is locked.
Why is fibromuscular dysplasia the lesion you actually fix with a balloon?
FMD is a non-inflammatory wall disease, not a plaque, sitting in the distal artery as a beaded segment. Stretching it open with a balloon restores flow, drops the renin-driven pressure, and often cures the hypertension, especially if it is young. FMD is the curable one: balloon the pipe, no routine stent.
Why not stent every atherosclerotic stenosis you see?
Because two large randomized trials showed routine stenting of stable atherosclerotic disease did not beat optimal medical therapy on blood pressure, kidney function, or major events. The narrowing is a marker of diffuse vascular disease best treated with meds and risk-factor control. Stenting a stable narrowing just because you see it, the oculostenotic reflex, is wrong.
Why does bilateral disease change everything about ACE inhibitors?
In bilateral stenosis (or a stenotic solitary kidney), the kidney cannot raise its inflow, so it holds filtration by using angiotensin II to constrict the efferent arteriole. Block that axis with an ACE inhibitor or ARB and the efferent dilates, intraglomerular pressure falls, and filtration drops. Bilateral RAS plus an ACE inhibitor equals a falling filtration rate and a climbing creatinine.
Two Diseases, Two Treatments
FMD and atherosclerosis: the management is opposite
Tap between them. Notice that the curable lesion gets a balloon and the diffuse-disease lesion gets medicine, and that a stent belongs to neither by reflex.
Fibromuscular dysplasia
Atherosclerotic
Fibromuscular dysplasia (FMD)
The curable one. Balloon the pipe.
The Treatment
Percutaneous balloon angioplasty (PTA), without a routine stent. Frequently curative of the hypertension, best when treated early.
When a stent goes in
Only to rescue a complication such as a dissection during the procedure. A stent is not the planned FMD treatment.
Who and where
Young to middle-aged woman. Narrowing in the distal two-thirds of the renal artery, with a beaded "string of beads" appearance.
📸 String of beads (FMD angiogram)
Catheter angiography of FMD: alternating dilations and webs give the beaded look in the distal artery. Tap to expand.
Role of medication
An ACE inhibitor or ARB controls the blood pressure, but it manages rather than cures. Angioplasty is what offers the cure.
Why it is fixable
FMD is a non-inflammatory wall problem, not a plaque. Stretching the segment open restores flow and drops the renin-driven pressure.
Board Trap
Do not reflex to a stent and do not settle for lifelong pills in FMD. Balloon the pipe; the hypertension may resolve for good.
One honest caveat: a few review sources describe FMD treatment as angioplasty with or without a stent and are cautious about calling it curable. The widely taught board line is balloon angioplasty without a routine stent, frequently curative when treated early. Do not memorize "stent the FMD," and do not memorize "FMD can never be cured."
Atherosclerotic renal artery stenosis
Diffuse disease. Treat the patient, not the picture.
First-line
Optimal medical therapy: an ACE inhibitor or ARB for the pressure, plus a statin, aspirin, smoking cessation, and glucose and lipid control.
Routine stenting
Adds no benefit over optimal medical therapy for blood pressure, renal function, or major events. Two large randomized trials established this.
When to revascularize
Reserve angioplasty with a stent for refractory hypertension, progressive renal decline, recurrent flash pulmonary edema, or true inability to tolerate medical therapy.
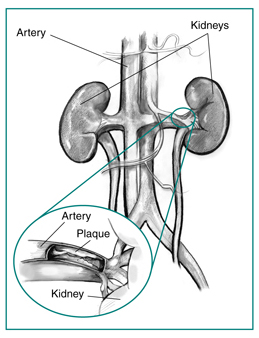
🟫 Ostial plaque (illustration)
Illustration: an atherosclerotic plaque at the renal artery origin. Ostial plaques recoil, which is why a stent is added when these are revascularized. Tap to expand.
Who and where
Older patient, often a male smoker. The plaque sits proximally or at the ostium, continuous with aortic disease.
If you do intervene
An ostial lesion gets angioplasty plus a stent, because the plaque recoils. Surgery (aortorenal bypass) is for complex anatomy or failed endovascular treatment.
Board Trap
The oculostenotic reflex, stenting a narrowing just because you see it, is wrong. A stenosis on imaging is not an indication to revascularize.
🖼️ CT angiography of the renal artery
CT angiography images the renal artery noninvasively. Imaging confirms and localizes the lesion, but the cause and the clinical picture, not the picture alone, decide the treatment. Tap to expand.
The Signature Tool
Best Next Step: route the patient, do not reflex to a stent
Five real crossroads. Commit to a management move before each reveal. The same narrowed artery can need opposite actions depending on the patient in front of you.
Renovascular Clinic · Decision Bay
ROUTE THE STENOSIS
Five patients · one narrowed artery each · five different right answers
A narrowed renal artery is not a diagnosis you treat the same way twice. Read the patient, commit to the next step, then see why.
Commit to the best next step before the reveal.
Routing complete
The five routes, locked
FMDBalloon angioplasty, no routine stent. Often curative.
Stable atheroOptimal medical therapy. Routine stenting adds nothing.
Cr up >30%Stop the ACE inhibitor or ARB. Suspect bilateral disease.
Flash edemaRevascularize (angioplasty + stent) the bilateral disease.
Untreated BPStart an ACE inhibitor or ARB, watch the creatinine.
Medical Therapy
ACE inhibitors and ARBs: first-line, and the bilateral trap
Renin-angiotensin blockade is the targeted drug for renovascular hypertension. In unilateral disease it is safe. In bilateral disease it can crash the filtration rate, and that is the highest-yield trap on this topic.
🧬 The renin-angiotensin-aldosterone system
A stenotic kidney senses low pressure and fires renin, driving angiotensin II. Angiotensin II constricts the efferent arteriole to defend filtration, which is exactly the support an ACE inhibitor or ARB removes. Tap to expand.
✅ Unilateral disease: ACE inhibitor or ARB is safe
With a normal contralateral kidney, blocking angiotensin II is effective and first-line for the renovascular hypertension. The healthy kidney maintains overall filtration. Start the drug and monitor creatinine and potassium.
Add a statin, aspirin, smoking cessation, and glucose and lipid control alongside.
⚠️ Bilateral disease: watch the creatinine
Both kidneys depend on angiotensin II to hold filtration, so renin-angiotensin blockade can drop the filtration rate. A creatinine rise greater than about 30% after starting an ACE inhibitor or ARB is the red flag. Hold the drug and suspect bilateral renal artery stenosis.
Same caution for stenosis of a solitary kidney.
The highest-yield trap
Creatinine up more than 30% the week you start an ACE inhibitor or ARB equals bilateral renal artery stenosis until proven otherwise. Stop the drug. Switching to the other class does not help, because both block the same axis. Monitor creatinine and potassium one to two weeks after any RAAS-blocker start or dose change.
Tap each line to reveal the mechanism and the monitoring.
How does an ACE inhibitor actually lower the pressure in renovascular hypertension?
The stenotic kidney sees low pressure and pumps out renin, raising angiotensin II, which clamps systemic vessels and the efferent arteriole. An ACE inhibitor cuts angiotensin II, relaxing those vessels and dropping the blood pressure. Less angiotensin II means less efferent constriction and a lower intraglomerular pressure.
So why does that same drug hurt a bilateral patient?
When both kidneys are stenosed, neither can raise its inflow, so each leans on angiotensin II to keep the efferent arteriole tight and hold filtration. Remove that support and the efferent dilates, intraglomerular pressure falls, and the filtration rate drops. In bilateral disease the filtration rate is angiotensin-II dependent, so blocking it causes acute kidney injury.
What else reduces long-term risk besides the blood pressure drug?
Atherosclerotic renal artery stenosis is a marker of diffuse vascular disease. A statin, an antiplatelet such as aspirin, smoking cessation, and tight glucose and lipid control lower the long-term cardiovascular and renal risk far more than stenting a stable narrowing does. Treat the whole vasculature, not just the renal artery you can see.
Decision Tool
To stent or not to stent
A stenosis on imaging is not, by itself, a reason to revascularize. Tap each scenario and decide before the verdict shows: does it warrant revascularization, or medical therapy and watching?
Commit to a call in your head, then tap to reveal the verdict and the one-line reason.
Revascularize Medical therapy / no stent
Stable 75% atherosclerotic stenosis, blood pressure at goal, creatinine steady for a year.
tap to decide & reveal
Medical therapy
Trials showed no benefit from routine stenting here. A stable, controlled narrowing is a meds case, not a stent case.
Resistant hypertension that stays high despite truly maximal medical therapy.
tap to decide & reveal
Revascularize
Refractory hypertension on maximal meds is an accepted indication. When optimal therapy fails, revascularization is on the table.
Progressive, rapidly declining renal function attributable to the stenosis (ischemic nephropathy).
tap to decide & reveal
Revascularize
Worsening kidney function from the lesion can justify opening it. A kidney failing because of the stenosis may warrant revascularization.
Recurrent flash pulmonary edema with bilateral disease, despite maximal therapy.
tap to decide & reveal
Revascularize
This is the classic bilateral indication. Recurrent flash edema with bilateral RAS is a revascularize answer.
A narrowing simply seen on imaging in a controlled, stable patient.
tap to decide & reveal
No stent
This is the oculostenotic reflex, and it is wrong. You do not stent a picture; you treat a patient.
True inability to tolerate medical therapy despite appropriate trials.
tap to decide & reveal
Revascularize
Genuine intolerance of medical therapy is an accepted reason. If the patient cannot take the meds, revascularization becomes reasonable.
Fibromuscular dysplasia with a beaded distal artery and resistant hypertension.
tap to decide & reveal
Balloon, no stent
FMD gets balloon angioplasty, often curative, and a stent only to rescue a complication. FMD is an angioplasty answer, not a stent answer.
Make it stick
Five hooks for the management traps
Tap each card to reveal the hook. These are built to survive a tired night before the exam.
🧶
FMD vs atherosclerosis
FMD: fix the pipe (balloon, often a cure). Atherosclerosis: treat the patient (meds), and stent only if it fails.
tap to reveal
🖼️
No reflex stenting
A stenosis on a scan is not a reason to stent. The large randomized trials said so. Treat a patient, not a picture.
tap to reveal
📉
The creatinine trap
Creatinine climbs more than 30% after an ACE inhibitor or ARB? You just unmasked bilateral renal artery stenosis. Pull the drug.
tap to reveal
✅
Unilateral is safe
Unilateral RAS: an ACE inhibitor or ARB is safe and first-line. Just watch the creatinine and potassium after you start.
tap to reveal
🔧
When to revascularize
Revascularize for refractory hypertension, failing kidneys, recurrent flash pulmonary edema, or true drug intolerance. Not for a picture.
tap to reveal
Board Walkthrough
The full clinical bank
Management vignettes. One at a time, shuffled, never repeats until the bank is exhausted. Right-click or long-press a choice to cross it out. Double-click or double-tap to highlight.
Vignette 1 of 6
Sources: Built from standard board-review physiology and emergency management of fluid and electrolyte disorders. Membrane-stabilization, transcellular shift, and elimination logic per general internal medicine and critical care references. All vignettes are original and rebuilt from mechanism.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.