A yellow nodule at the tip, nests of monotonous cells, markers lighting up in gold. Run the immunostain and you will never miss this one again.
The Immunostain
Run the Stain
Those small round blue cells fooled you into thinking lymphoma. Run the immunostain and see what they are really made of.
Immunohistochemistry
NE Marker Panel
A biopsy core with nests of monotonous cells. Run the marker panel to reveal the true identity.
Chromogranin A
--
Synaptophysin
--
CD56
--
CD20
--
CD45
--
RouteNests + rosettes + salt-and-pepper chromatin → granules store peptides → chromogranin/synaptophysin/CD56 label the granules
PatternNE markers = neuroendocrine. CD20/CD45 = lymphoid. They cannot both be true.
PearlSee chromogranin or synaptophysin? The answer is never a lymphoma.
🔢The appendix is the most common GI site for carcinoid tumors. Most are found incidentally at the tip, are under 2 cm, and have an excellent prognosis after appendectomy. Metastasis is rare at that size.
1 / 5
The Lineup
What Is This Lesion?
Five suspects, one answer. Tap each card to flip and see the rule that eliminates or confirms it.
⭐
Carcinoid (NET)
CORRECT ANSWER
Yellow nodule at the tip. Nests and rosettes. NE markers positive. Low-grade malignancy.
tap for board clues →
Appendiceal NET / Carcinoid
Gross:yellow-tan nodule at the tip, firm, usually <2 cm
Histo: nests, ribbons, and rosettes of monotonous round cells with salt-and-pepper chromatin
No discrete nests, no rosettes, no monotonous epithelioid cells
NE markers (chromogranin, synaptophysin): negative in reactive inflammation
No vasoactive peptide secretion
Organized nests with NE markers = neoplasm. Reactive tissue cannot produce this picture.
📐
Mucosal Dysplasia
EASY ELIMINATE
Architectural and cytologic atypia of surface epithelium. Not NE cells.
tap to flip →
Why Dysplasia Is Eliminated
Dysplasia = abnormal architecture and nuclear changes in surface epithelium
No formation of nests or rosettes in the submucosa
NE markers: negative (dysplasia is not neuroendocrine differentiation)
Yellow gross appearance and submucosal nodule do NOT fit dysplasia
Yellow submucosal nodule + NE markers = carcinoid. Surface dysplasia cannot explain this picture.
Board Trap: The small round blue cells of a carcinoid look IDENTICAL to lymphoma cells on a plain H&E stain. The board ALWAYS gives you the IHC panel in the stem. When you see
chromogranin AChromogranin A: a protein stored in dense-core secretory granules of NE cells. Positive IHC staining is the hallmark of any neuroendocrine tumor, from appendiceal carcinoids to pheochromocytomas to islet cell tumors.,
synaptophysinSynaptophysin: a membrane glycoprotein found in presynaptic vesicles and NE cell secretory vesicles. Positive in all NE tumors. The pair chromogranin + synaptophysin = NE differentiation, full stop., or
CD56CD56 (NCAM): a neural cell adhesion molecule expressed on natural killer cells AND NE cells. In the context of a GI tumor with nests and rosettes, CD56+ means NE tumor, not NK cell lymphoma.:
the answer is NEUROENDOCRINE. The lymphoma option is the trap.
2 / 5
The Syndrome Gate
When Does Carcinoid Syndrome Happen?
This is the most tested concept about carcinoids. Work through it step by step before the answer is revealed.
Step 1 of 3 · The Primary Tumor
A 35-year-old woman has a 1.4 cm carcinoid at the appendiceal tip, found incidentally during an appendectomy for appendicitis. She has no flushing, diarrhea, or wheezing. Her 5-HIAA is normal. Why does she NOT have carcinoid syndrome?
Small carcinoids CAN make serotonin. Size is not the reason. The barrier is where the venous blood drains, not the tumor's production capacity. Small carcinoids produce serotonin; the liver metabolizes it before it reaches the systemic veins.
Exactly right. The portal venous system drains the appendix and carries serotonin directly to the liver. The liver's MAO enzyme inactivates serotonin and converts it to 5-HIAA. Without hepatic mets to bypass this step, the serotonin never reaches systemic blood. No systemic serotonin = no carcinoid syndrome.
The appendix drains into the ileocolic vein and into the portal system, just like the rest of the GI tract. What matters is where the blood GOES after it leaves: straight to the liver. The hepatic portal system is the filter.
Size correlates with metastatic risk, not with whether carcinoid syndrome occurs. The trigger for carcinoid syndrome is hepatic metastasis, not tumor size. Carcinoid syndrome = hepatic mets, not large primary tumor.
Step 2 of 3 · Hepatic Metastasis
Four years later, CT shows four hepatic lesions. The patient now has episodic facial flushing and 8 loose stools per day. Which of the following best explains why the syndrome appeared now?
Volume is not the answer. The primary tumor was already producing serotonin for years. What changed is WHERE the serotonin drains, not HOW MUCH is made. Route beats volume: mets drain into hepatic veins, bypassing the MAO filter.
Correct mechanism. Hepatic mets are inside the liver. Their venous drainage goes into hepatic veins, directly into the IVC, right heart, and systemic circulation. The liver's MAO cannot catch serotonin that drains THROUGH the liver into hepatic veins. The first-pass gate is bypassed. Now serotonin causes flushing, diarrhea, and right-sided valve disease.
IVC compression causes edema and venous congestion, but NOT the carcinoid syndrome triad. Carcinoid syndrome is hormonal, not mechanical. Carcinoid syndrome is hormonal, not mechanical.
Hypoalbuminemia causes edema, not flushing and diarrhea. Liver failure would cause jaundice, coagulopathy, and encephalopathy. These are completely separate processes. Albumin is not the mechanism here.
Step 3 of 3 · Lock the Pattern
Echocardiography is ordered. Which cardiac finding is MOST specific to carcinoid syndrome?
Mitral stenosis is left-sided. Think about which side sees serotonin first: it enters systemic veins, flows to the right heart, hits tricuspid and pulmonic valves, then reaches the lungs where MAO inactivates it. Carcinoid spares the left side because the lungs inactivate serotonin before it reaches left-sided valves.
Aortic regurgitation is left-sided. Same reasoning: serotonin is inactivated in the pulmonary vasculature before it can damage the left side. The left-sided valves see almost no serotonin. Aortic and mitral = left side = protected by pulmonary MAO in carcinoid.
Correct. The sequence: hepatic met serotonin → hepatic veins → IVC → right atrium → right ventricle → tricuspid and pulmonic valves (DAMAGED) → pulmonary circulation (MAO inactivates serotonin) → left side (mostly spared). Right-sided valve disease is the carcinoid cardiac signature. Measure urinary 5-HIAA to confirm.
Pericardial effusion is not a carcinoid syndrome feature. Carcinoid fibrosis targets the endocardium of the right-sided valves, not the pericardium. Carcinoid = valve fibrosis, not pericardial disease.
🌞The Carcinoid Quartet:Flushing, Diarrhea, Wheezing, Right-sided heart fibrosis. You only get this quartet when serotonin has escaped the liver. Diagnose with 24-hour urinary 5-HIAA5-hydroxyindoleacetic acid: the major urinary metabolite of serotonin. Elevated in carcinoid syndrome. Measure in a 24-hour urine collection.. Treat with octreotideOctreotide: a synthetic somatostatin analog. Binds somatostatin receptors on NE tumor cells and suppresses secretion of serotonin and other vasoactive peptides. First-line symptomatic treatment for carcinoid syndrome..
3 / 5
Evidence Locker
Lock the Pattern
Four hooks. Tap to reveal. Read once, then close your eyes and say it back.
Hook 1 · The Yellow Clue
Why is the color yellow important?
NE cells store peptides in dense-core secretory granules. Those granules are slightly lipid-rich and lipochrome-pigmented. That is why carcinoid tumors appear yellow-tan on gross inspection. No other common appendiceal mass is yellow. Adenocarcinoma is white-gray. Lymphoma is white-pink. GIST is white-gray. Yellow = carcinoid.
tap to reveal
Hook 2 · The First-Pass Gate
Why does carcinoid syndrome require liver mets?
Think of the liver as a security checkpoint. Every GI vein drains into the portal system, which goes straight to the liver before anything gets into general circulation. The liver's MAO shreds serotonin at this checkpoint. Only serotonin that is ALREADY INSIDE the liver can bypass the checkpoint by draining via hepatic veins. Hepatic mets are the only way to sneak serotonin past the liver.
tap to reveal
Hook 3 · Right Not Left
Why does carcinoid hit the right side of the heart?
Systemic serotonin returns to the heart through the inferior vena cava and flows into the right atrium first. Then the right ventricle. Then the pulmonary vasculature, which has its own MAO. The lungs inactivate the serotonin before it exits into the pulmonary veins. So the left side (mitral, aortic) is mostly protected. Pulmonic stenosis + tricuspid regurgitation is the carcinoid cardiac signature.
tap to reveal
Hook 4 · Size and Prognosis
When is an appendiceal carcinoid dangerous?
Almost never. Under 2 cm: appendectomy is curative, metastasis risk under 2%. Over 2 cm: the metastatic risk jumps to around 30%. Most incidental appendiceal carcinoids are 1 to 1.5 cm and found during appendectomy for appendicitis. The board will try to make you panic by calling it "malignancy." The correct management for sub-2-cm lesions with clear margins is appendectomy alone.
tap to reveal
Clinical Images
What You Are Actually Seeing
Tap any image to enlarge. Recognize these on exam day.
📷 Gross Pathology · Appendiceal Tip
📷 H&E · Nests of Monotonous Cells
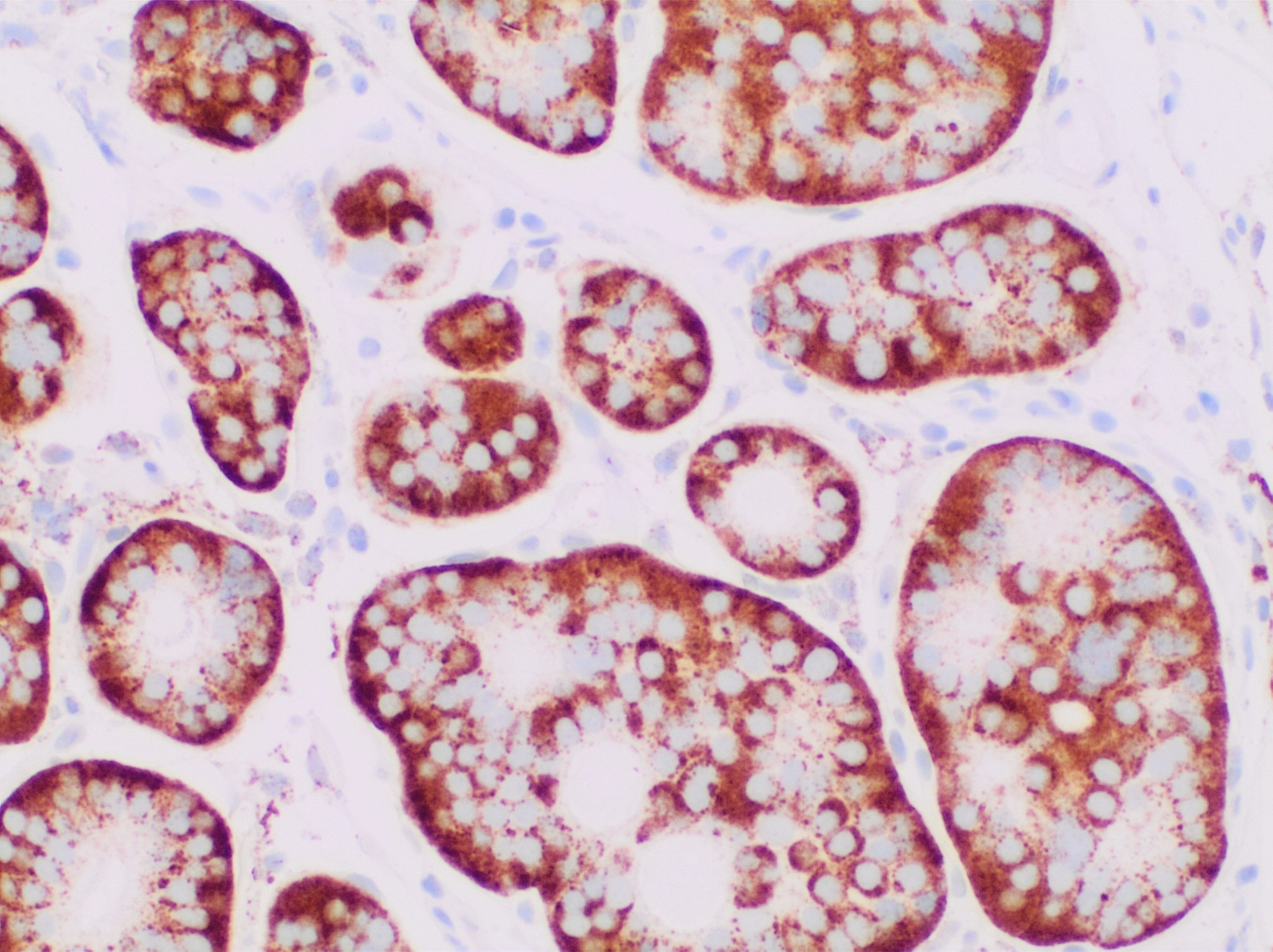
📷 IHC · Chromogranin A Positive
Appendiceal Carcinoid · Gross PathologyThe classic yellow-tan firm nodule at the appendiceal tip. Under 2 cm in most incidental cases. The yellow color comes from lipochrome pigment in the NE secretory granules. This appearance is nearly pathognomonic for a carcinoid/NET.Wikimedia Commons, CC BY-SA 3.0
Appendiceal Carcinoid · H&E HistologyNests, ribbons, and cords of monotonous round-to-oval cells with granular pale cytoplasm and fine salt-and-pepper chromatin. No significant mitotic activity in low-grade tumors. This pattern is the morphologic signature of a well-differentiated NET.Wikimedia Commons, CC BY 4.0
Chromogranin A · IHC Stain (Positive)Brown cytoplasmic staining (DAB chromogen) marking chromogranin A in the secretory granules of NE cells. This is the single most reliable IHC marker for NE differentiation. A lymphoma would be entirely negative here.Wikimedia Commons, CC0
Board Trap: A carcinoid is technically a low-grade malignancy. Boards love to offer "benign adenoma" as a wrong answer. A carcinoid is NOT benign: it can metastasize (especially over 2 cm). The correct framing is "low-grade malignancy with excellent prognosis if under 2 cm." The correct management answer is almost always simple appendectomy for the incidental sub-2-cm tip lesion.
4 / 5
Board Walkthrough
See If It Stuck
Eight original vignettes, served in shuffled order. Confetti reserved for correct first attempts.
The pool shuffles on load and never repeats until you exhaust the full set. Tap any explanation to see it beat by beat.