Hodgkin vs NHL, Reed-Sternberg cells, and the translocations that define each subtype
Opener Challenge
A 28-year-old man presents with painless cervical lymphadenopathy, night sweats, and a 10-pound weight loss over 2 months. CT shows mediastinal lymphadenopathy. Biopsy reveals large binucleated cells with prominent "owl-eye" nucleoli surrounded by reactive inflammatory cells. What is the diagnosis?
Diffuse Large B-Cell Lymphoma
Hodgkin Lymphoma
Burkitt Lymphoma
Follicular Lymphoma
Reed-Sternberg cells (large binucleated with owl-eye nucleoli) are pathognomonic for Hodgkin lymphoma. Young adult + mediastinal involvement + B symptoms (fever, night sweats, weight loss greater than 10% in 6 months) = classic HL. No other lymphoma has RS cells.
Section 1
Hodgkin Lymphoma
Reed-Sternberg cells, B symptoms, and the ABVD regimen
Classic Hodgkin
Subtypes
Pathognomonic Cell
Reed-Sternberg Cell
Immunophenotype
CD15+ · CD30+ · CD45-
Age Distribution
Bimodal: 15-35 & >55
Spread Pattern
Contiguous (predictable)
B Symptoms (prognostic): Fever >38°C, drenching night sweats, weight loss >10% body weight in 6 months. Presence = worse prognosis, upstages treatment intensity.
Staging: Ann Arbor I-IV. Stage I = single node region. Stage II = 2+ regions same side of diaphragm. Stage III = both sides of diaphragm. Stage IV = extranodal spread. Add "B" if B symptoms present.
Mediastinal involvement is common in HL, especially Nodular Sclerosis subtype. CT chest is mandatory. Bulky mediastinal disease (>1/3 chest width) = adverse prognosis.
Nodular Sclerosis
Most common subtype (70%). Young women, mediastinal mass. Lacunar cells (RS cell variant in formalin). Collagen bands divide nodes into nodules. Best overall prognosis among classic HL subtypes.
Most CommonYoung WomenMediastinal
Mixed Cellularity
Older men, many classic RS cells in mixed inflammatory background. HIV-associated. Second most common. Intermediate prognosis.
Older MenHIV-associated
Lymphocyte-Rich
Rare. Few RS cells, abundant lymphocytes. Best prognosis among classic HL subtypes. Presents in older men, localized disease.
Best Prognosis
Lymphocyte-Depleted
Rare, aggressive. Many RS cells, very few lymphocytes. Associated with AIDS and elderly. Worst prognosis among classic HL.
Worst PrognosisAIDS-associated
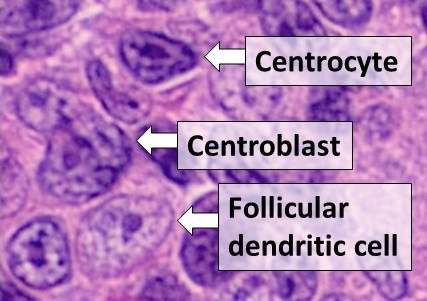
Nodular Lymphocyte Predominant (NLPHL)
Distinct from classic HL. Popcorn cells (lymphocytic and histiocytic [L&H] cells) instead of classic RS cells. Immunophenotype: CD20+, CD15-, CD30- (opposite of classic HL). Best prognosis overall. Treated differently (anti-CD20 rituximab-based).
CD20+CD15- · CD30-Best Prognosis
High-yield memory: NS = most common (No Sweat, 70%). LC = least bad. LD = most bad (L = Last). NLPHL = popcorn cells + CD20+ = treat like NHL, not classic HL.
Section 2
Non-Hodgkin Lymphoma
Four major subtypes with distinct translocations, behaviors, and treatments
NHL is far more common than HL. Most are B-cell origin. Unlike HL, spread is non-contiguous (unpredictable). Key board question pattern: match the translocation to the subtype.
Diffuse Large B-Cell LymphomaTAP
Most common NHL overall. Aggressive, fast-growing. Rapidly enlarging lymph node mass.
Immunophenotype: CD20+. BCL-6 or BCL-2 rearrangements (multiple mechanisms).
Treatment: R-CHOP (Rituximab + Cyclophosphamide + Hydroxydaunorubicin/doxorubicin + Vincristine/Oncovin + Prednisone). Curable in approximately 60%. CNS prophylaxis if high-risk (double-hit lymphoma, elevated LDH, extranodal disease).
Most Common NHLCD20+R-CHOPAggressive
Follicular LymphomaTAP
Second most common NHL. Indolent (slow-growing), but incurable with standard therapy. "Waxing and waning" lymphadenopathy is classic.
Translocation: t(14;18) moves BCL-2 next to the IgH locus, causing BCL-2 overexpression. BCL-2 is anti-apoptotic, so B cells avoid programmed death and accumulate.
Immunophenotype: CD10+, CD20+. Treatment: watch and wait if asymptomatic. R-CHOP or rituximab when symptomatic. Can transform to DLBCL (Richter-like transformation, 3%/year).
t(14;18)BCL-2IndolentIncurable
Burkitt LymphomaTAP
Fastest-growing human cancer (doubling time approx. 24 hours, highest Ki-67 of any tumor). Very aggressive.
Translocation: t(8;14) moves c-MYC next to IgH locus, causing c-MYC overexpression, which drives uncontrolled proliferation.
Three clinical forms: Endemic (African children, jaw mass, EBV-associated), Sporadic (abdominal mass, Western children/young adults), Immunodeficiency-related (HIV).
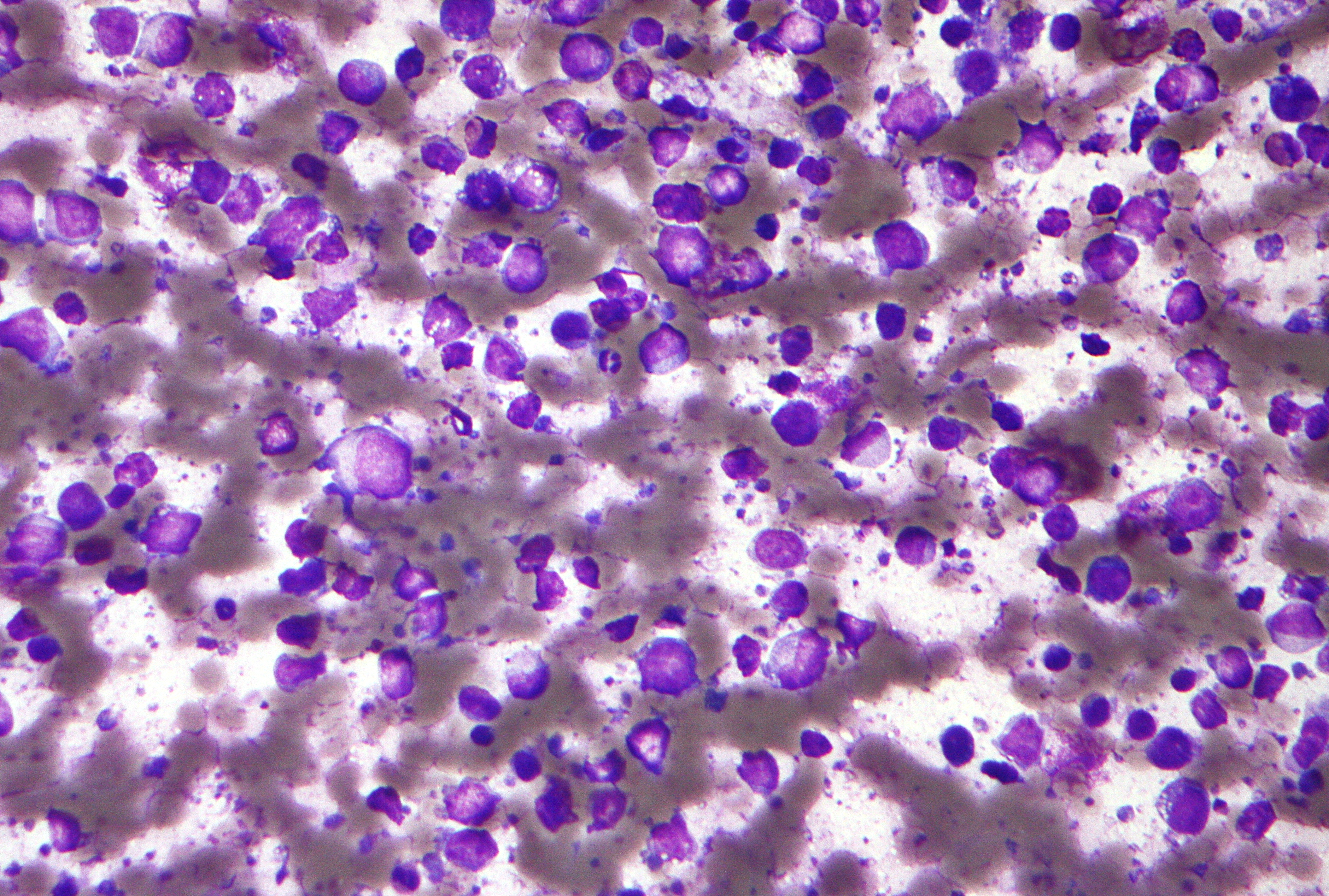
Histology: "Starry sky" pattern = macrophages with apoptotic debris (stars) against dark sea of lymphocytes. Treatment: aggressive hyper-CVAD or CODOX-M/IVAC.
t(8;14)c-MYCStarry SkyFastest Growth
Mantle Cell LymphomaTAP
Aggressive B-cell lymphoma, classic in middle-aged men. Widespread lymphadenopathy, splenomegaly, GI involvement (lymphomatous polyposis of colon).
Translocation: t(11;14) moves cyclin D1 next to IgH locus. Cyclin D1 overexpression drives cells through the G1/S checkpoint, bypassing normal cell cycle brakes.
ALK fusion protein, T-cell lymphoma, ALK inhibitors active
t(11;18)
API2-MALT1
MALT Lymphoma
Anti-apoptotic NF-kB signaling, H. pylori-associated gastric form
The three you must own: t(14;18) = Follicular (BCL-2, anti-apoptotic). t(8;14) = Burkitt (c-MYC, proliferation). t(11;14) = Mantle Cell (Cyclin D1, G1/S bypass). Each translocation names the gene partner; each gene names the mechanism.
Burkitt grows fastest. Follicular grows slowest. Both are B-cell. Both involve chromosome 14 (IgH locus). The partner chromosome tells you which gene gets hijacked: 18 = BCL-2 (survival), 8 = MYC (growth), 11 = Cyclin D1 (cell cycle).
BCL-2 mnemonic: "B-cells Cling on to Life 2 long" (follicular: indolent, won't die). MYC mnemonic: "My Cell grows" (Burkitt: maximal proliferation). Cyclin D1: "D1 = Done before the checkpoint" (mantle cell bypasses G1 brake).
The Forge. Each translocation swaps a chromosome arm onto the immunoglobulin heavy chain (IgH) locus on chromosome 14. Tap a translocation and watch the partner arm fuse onto 14. The hijacked gene falls under the IgH enhancer and gets overexpressed. The gene tells you the mechanism; the mechanism tells you the lymphoma.
t(14;18)
t(8;14)
t(11;14)
t(11;18)
14IgH
18
der(14)
partner
Diagnostic fork. Two nodes. Read the clue, commit to a branch, then reveal. Tap an answer to lock it in.
Node 1 of 2 · Is it Hodgkin?
A nodal biopsy shows large binucleated cells with owl-eye nucleoli on a reactive background of lymphocytes, eosinophils, and plasma cells. Immunostains: CD15+, CD30+, CD45 negative, CD20 negative. Which branch do you take?
AHodgkin branch: these are Reed-Sternberg cells
BNon-Hodgkin branch: this is a CD20+ B-cell lymphoma
Hodgkin branch. CD15+ CD30+ CD45 negative on owl-eye binucleated giants is the Reed-Sternberg fingerprint. The cells came from germinal center B cells but shed CD20 and CD45 during transformation, so the CD20-negative result is expected, not a redirect to NHL. Reactive eosinophils and plasma cells surrounding scarce tumor cells seal it. Break it down: owl-eye binucleated cells that are CD15+/CD30+/CD45 negative are Reed-Sternberg cells, so take the Hodgkin branch even when CD20 is negative.
Node 2 of 2 · Which NHL by translocation?
A different patient: a young man with an explosive jaw mass, a biopsy showing a starry sky pattern of macrophages engulfing apoptotic cells, and a near-100% Ki-67. Cytogenetics return a chromosome 8 to chromosome 14 swap. Which branch do you take?
Burkitt branch. A chromosome 8 to 14 swap puts c-MYC under the IgH enhancer, and c-MYC is the master proliferation driver behind the fastest doubling time of any human cancer. Starry sky plus near-100% Ki-67 plus a jaw mass in a young patient is the endemic Burkitt signature. t(14;18) would give BCL-2 and an indolent follicular course, which is the opposite tempo. Break it down: a chromosome 8 to 14 swap is c-MYC driven Burkitt, so high Ki-67 with a starry sky takes the Burkitt branch, never the indolent follicular branch.
Section 4
Elimination Game
Use the clues to eliminate wrong answers. One lymphoma survives.
A 35-year-old man presents with a rapidly enlarging abdominal mass and jaw swelling. LDH is markedly elevated. Biopsy shows a "starry sky" pattern. Cytogenetics reveal t(8;14).
Hodgkin Lymphoma
Follicular Lymphoma
Burkitt Lymphoma
Mantle Cell Lymphoma
Clue 1: "Starry sky" histology is caused by macrophages engulfing apoptotic tumor cells, creating pale stars against a dark lymphocyte background. This pattern is characteristic of Burkitt lymphoma. Hodgkin lymphoma shows Reed-Sternberg cells (owl-eye nucleoli) in a reactive background, not starry sky. Follicular lymphoma shows follicular (nodular) architecture, not starry sky.
Clue 2: Cytogenetics show t(8;14), placing c-MYC next to the IgH enhancer. This drives maximal proliferation, explaining the 24-hour doubling time and markedly elevated LDH. Mantle cell lymphoma shows t(11;14)/cyclin D1, not t(8;14). The jaw mass in a young man + abdominal mass = endemic or sporadic Burkitt pattern.
Burkitt Lymphoma
t(8;14), starry sky, jaw mass, rapidly enlarging abdominal mass, very high LDH = Burkitt. Every clue points here. Fastest-growing cancer, c-MYC driven, treat aggressively. Watch for tumor lysis syndrome on initiation of chemo.
Section 5
Board Walkthrough
25 clinical vignettes. One at a time. Shuffle to mix the order.
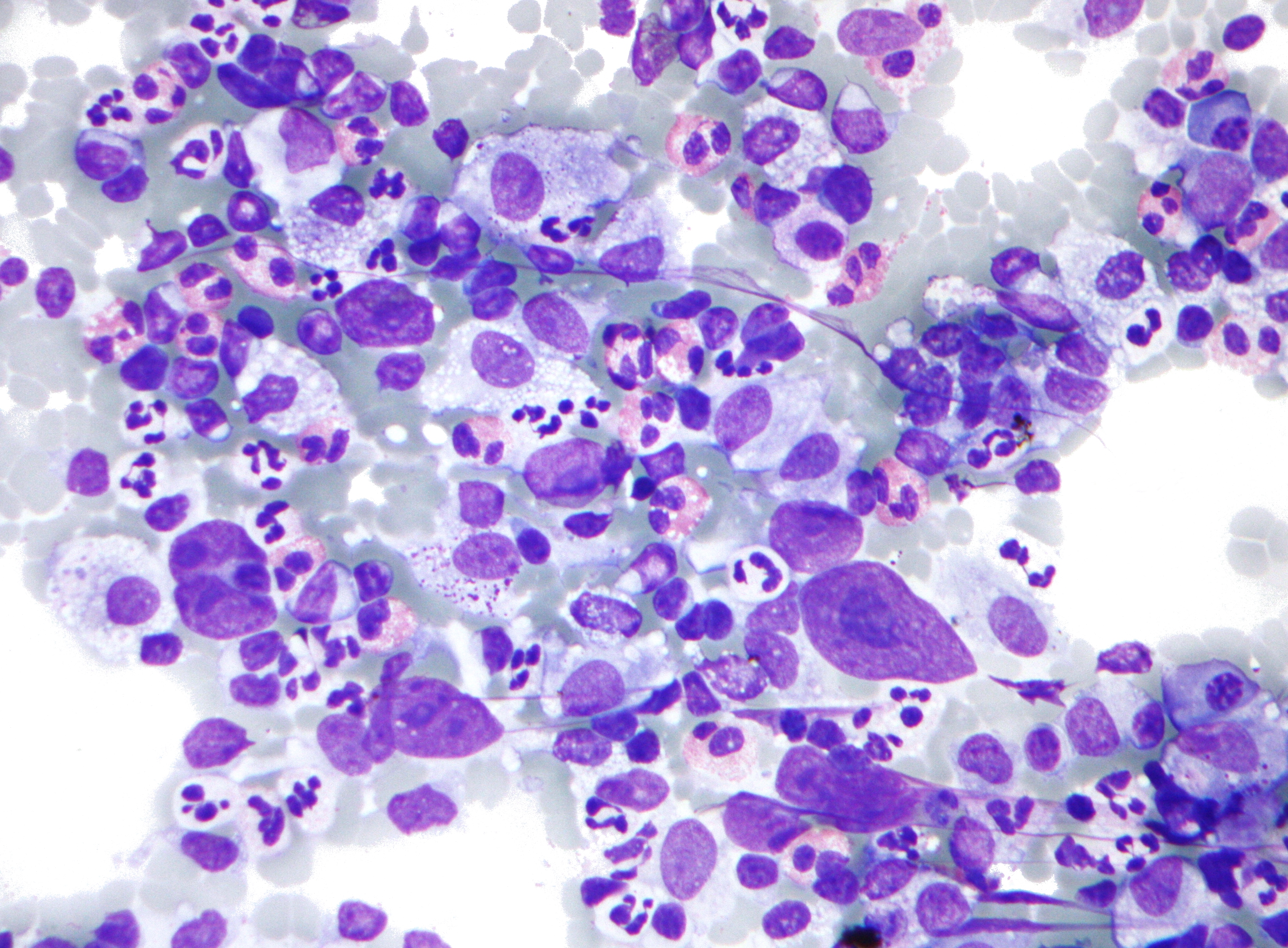
RS Cell H&E
Burkitt Starry Sky
Follicular Lymphoma
DLBCL Large Cells
Q 1 / 250 correct
Section 6
Memory Hooks
The sticky one-liners that survive exam-day stress. Anchor each clue to its lymphoma.
Owl eyes
Binucleated owl-eye cell equals Reed-Sternberg equals Hodgkin. CD15+ and CD30+, but CD45 negative. The badge it kept (CD30) is the one brentuximab hunts.
Starry sky
Stars in the sky equals macrophages eating apoptotic cells equals Burkitt. t(8;14), c-MYC, fastest cancer alive. Pretreat for tumor lysis before chemo.
Cling on 2 long
"B-cells Cling on to Life 2 long" equals BCL-2 equals Follicular, t(14;18). Anti-apoptotic, indolent, waxes and wanes, incurable but slow.
Done before the checkpoint
Cyclin D1 equals "Done before the G1 checkpoint" equals Mantle cell, t(11;14). CD5+ like CLL, but CD23 negative and cyclin D1 positive.
Popcorn
Popcorn cells that are CD20+ and CD45+ equals NLPHL. It keeps its B-cell badges, so rituximab works and the prognosis is the best of the bunch.
Bacteria first
Stomach lymphoid lesion plus H. pylori equals gastric MALT. Eradicate the bug first; up to 80% regress. t(11;18) cases resist and need radiation.
Keep the momentum
You just locked in lymphoma pattern recognition. Carry the streak into the next high-yield heme topic.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.