Every transmitter is a triad: where it is made, what it does, and the disease when it swings. Acetylcholine down means memory. Dopamine down means movement. Learn the swing, then own the four dopamine pathways and the drugs that ride the chloride channel.
Start where most people slip. Boards rarely ask a transmitter by name. They hand you a disease and make you name the transmitter that fell, or the one that surged. Read the patient, then call the swing.
Why this trips people: two of the most-tested diseases both cause memory or movement problems in older adults, so it is easy to grab the wrong transmitter. The trick is the direction and the site: which chemical fell, and where it is made.
A 72-year-old man is brought to the clinic by his daughter because of 2 years of worsening forgetfulness. He gets lost in his own neighborhood and repeats questions within minutes. There is no tremor and no rigidity. On exam he is alert but cannot recall 3 objects at 5 minutes. An autopsy years later would show degeneration of the basal nucleus of Meynert.
Loss of which neurotransmitter best explains his memory decline?
Acetylcholine down means memory. The basal nucleus of Meynert is the cholinergic hub that dies in Alzheimer disease.
Dopamine felt tempting because it is the other famous "old person's brain chemical," but dopamine loss gives a movement problem (tremor, rigidity, Parkinson), and this man has no tremor and no rigidity. Serotonin and norepinephrine track mood, not this kind of amnesia. GABA loss lowers the seizure threshold, not memory. The named site, the basal nucleus of Meynert, is the tell: it is the source of cortical acetylcholine, so when it dies, memory goes with it. That is also why we reach for acetylcholinesterase inhibitors like donepezil to prop the acetylcholine back up.
One transmitter, three facts
The whole page runs on one shape. Learn every transmitter as this triad and the diseases fall out for free.
1
Site
Where it is made. A named nucleus is a free answer.
2
Function
What it does when it fires normally.
3
Disease
The classic illness when it swings up or down.
Site → Function → Disease. Read it left to right, every time.
1 / 6
The Messenger Board
Tap a source on the brain. Its transmitter, function, and classic disease appear on the right as one triad. These are the seven the boards return to again and again.
Tap a colored source on the brain to reveal its transmitter, what it does, and the disease it drives.
The synapse in one picture: release, cross the cleft, bind. Tap to enlarge.
Side by side: the seven
Tab through each one. Read the swing arrow on the disease row: the color tells you up or down.
2 / 6
The Dopamine Circuit Board
Dopamine runs four wires out of the midbrain, and the boards test what happens when a drug cuts each one. Tap a wire, predict the result of blocking its D2 receptors, then reveal. Guess before you look.
Tap one of the four dopamine wires. You will be asked to predict what happens when a drug blocks its D2 receptors, then the answer opens.
The substantia nigra: the dopamine source that dies in Parkinson. Tap to enlarge.
The clean way to hold all four: a single dopamine blocker (an antipsychotic) does four things at once. It calms the mesolimbic wire (good, treats hallucinations), starves the nigrostriatal wire (bad, causes stiffness and tremor), worsens the mesocortical wire (bad, flattens motivation), and frees the tuberoinfundibular wire (bad, raises prolactin). One drug, four wires, four consequences.
3 / 6
The Channel Gate
Two patients overdose on two different sedatives. Both drugs open the same chloride gate, but in two different ways. Watch the gate, then call which drug did it. This one wins points every exam.
The Consult
Marcus
Age 24 · Two sedatives, one gate
"He took his sister's anxiety pills. He is sleepy but wakes to voice and his breathing is fine. Down the hall, another patient took an old seizure barbiturate and is barely breathing. Same channel. Different gate."
Watch the chloride gate
Marcus is only lightly sedated: the gate flicks open and shut many quick times. Which drug opens the gate MORE OFTEN?
Pattern Locked
Frequency vs Duration
BenzoOpens the gate MORE OFTEN. Frequency. Needs GABA present to work.
BarbiturateHolds the gate open LONGER. Duration. Can open it even without GABA.
Why it mattersBarbiturates flatten breathing harder in overdose, because they force the gate open on their own. Benzos have a ceiling.
Marcus took a benzodiazepine: frequent quick openings, breathing preserved. The barbiturate patient down the hall held the gate open too long.
Two confusion pairs, side by side
The two look-alike pairs that cost points, both faces on the surface: how the sedatives differ, and how strychnine differs from tetanus.
Benzo vs Barbiturate
Same gate, two dials
Both boost the GABA-A chloride channel. One turns a frequency dial, the other a duration dial.
Benzo = Frequency (B and F, more openings)
Barbiturate = Duration (longer openings)
Barb can open the gate with NO GABA
That is why barbiturate overdose stops breathing
Strychnine vs Tetanus
Both hit glycine, differently
Both remove inhibition in the spinal cord and cause rigidity. But one blocks the receptor and one blocks the release.
Strychnine blocks the glycine RECEPTOR
Tetanus toxin blocks glycine and GABA RELEASE
Receptor blocked vs release blocked
Both leave motor neurons with no brakes
Excitatory or inhibitory?
The whole nervous system is a tug of war between two teams. Know which transmitter plays for which side.
Excitatory (gas pedal)
Glutamate: the main excitatory transmitter of the brain
Aspartate: the other excitatory amino acid
Inhibitory (brake pedal)
GABA: the main brake in the brain
Glycine: the main brake in the spinal cord
GABA is the brain brake, glycine is the cord brake. Glutamate is the gas. Lose a brake and you seize or spasm. Push the gas too hard after a stroke and you get excitotoxicity, which is why memantine (an NMDA blocker) exists.
4 / 6
Sort the Toxins
Boards love a poison. Walk one decision tree with the answer hidden until you commit, tap the drug cards to reveal each target, then lock the hooks.
A patient is rigid, with severe painful muscle spasms and a clenched jaw, after stepping on a rusty nail 8 days ago. There is no seizure activity on EEG and the patient is fully awake between spasms. The toxin is removing inhibition in the spinal cord. Guess the mechanism before it opens.
Which best explains the loss of inhibition in this patient?
Receptor blocked
Think strychnine. It sits on the glycine receptor so glycine is released but cannot brake. Awake, arched, spasming.
Release blocked
Think tetanus toxin. It cleaves SNARE proteins so inhibitory glycine and GABA never leave the neuron. Lockjaw, risus sardonicus.
Na channel blocked
Think tetrodotoxin or a local anesthetic. That stops nerve conduction entirely (numbness, weakness), not a spasm.
Tetanus blocks the release, strychnine blocks the receptor. Rusty nail plus lockjaw is tetanus. Same end result, no brakes, but the level of the block is the whole question.
Drug and toxin targets
Tap a card to reveal its target and the one-line consequence. Test yourself first.
Hooks that stick
Tap each card to unblur the hook. These are built to survive the test.
5 / 6
See it, then drill it
Ground the abstractions in real tissue and real signs, then run the board bank until the swings are automatic.
On real patients and tissue
Tap any image to enlarge. Each one is a transmitter story you can see.
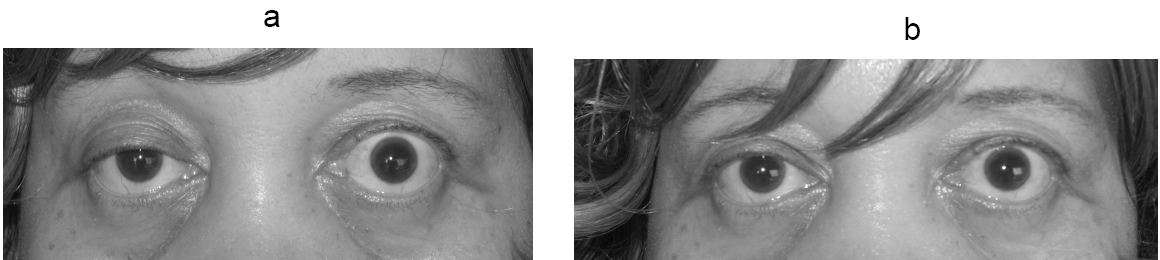
ACh receptor · myasthenia
Nicotinic ACh receptor blocked by antibody. Weakness that a cholinesterase inhibitor reverses.
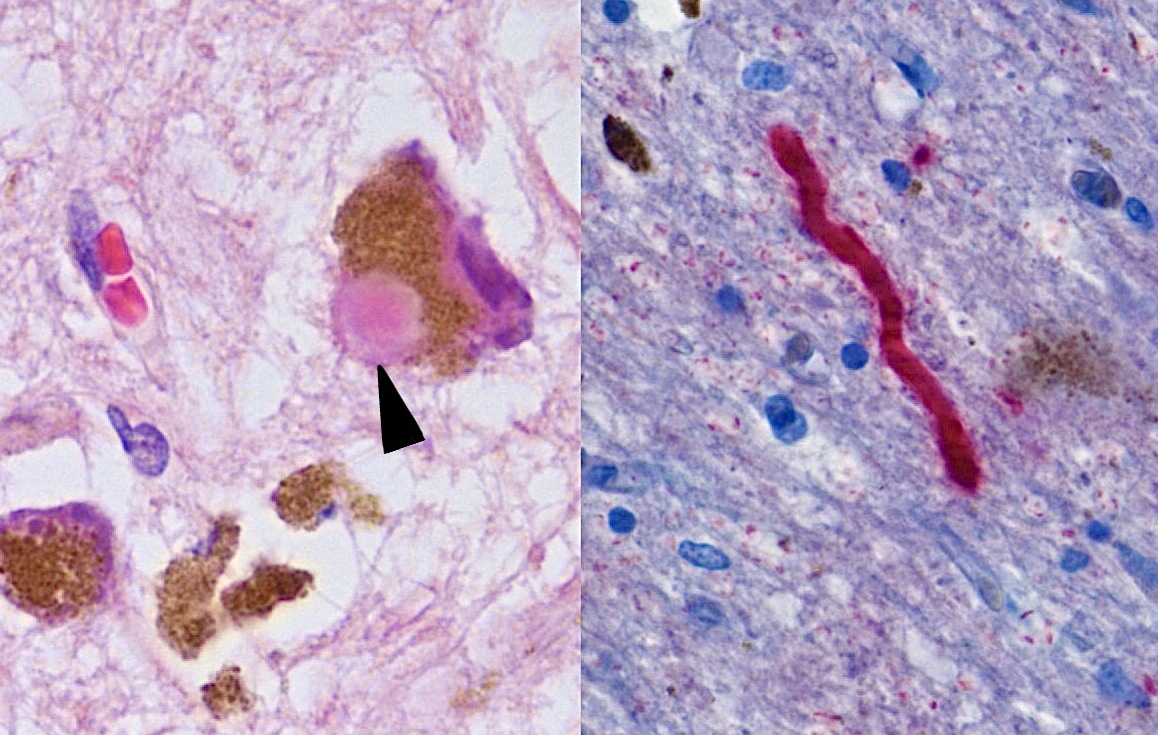
Dopamine loss · Parkinson
A Lewy body in a dying dopamine cell. Fewer cells, less dopamine, more tremor.
ACh · neuromuscular junction
Where acetylcholine meets muscle. The junction myasthenia attacks.
Dopamine source · midbrain
Pale substantia nigra. The dopamine factory, shut down.
The board bank
One vignette at a time. Right-click or long-press a choice to cross it out. Double-click or double-tap to highlight it. Choices and cases shuffle, and nothing repeats until the bank is empty.
Case 1 / 26Neurotransmitters
Tip: cross out the answers you have killed, highlight the one you are torn on, then commit.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed July 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.