Drag the slider. Eight steps from vessel injury to a stable cross-linked fibrin clot. Each step lights up the molecule responsible and the drug that blocks it.
Endothelium ruptures. Subendothelial collagen + tissue factor are exposed to flowing blood. The clot has not formed yet · the body is about to launch two parallel responses (vasoconstriction + platelet plug) within seconds.
Hemostasis is two parallel responses to one injury. Primary (vasoconstriction + platelet plug) happens in seconds · secondary (cascade → fibrin) takes minutes. Where bleeding shows up tells you which is broken: mucocutaneous (gums, nose, petechiae, menorrhagia) = primary defect. Deep + delayed (hemarthrosis, intramuscular, intracranial) = secondary defect. Build the clot once in your head; every bleeding stem is asking which step broke.
Tap through five stages. Watch the cascade assemble from tissue injury to stable fibrin.
Endothelium breaks. Tissue factor and collagen are now exposed to blood. This is the starting gun for both the extrinsic and intrinsic pathways.
Two pathways, one finish line. Extrinsic (tissue factor + VII) is fast and measured by PT. Intrinsic (XII, XI, IX, VIII) is slower and measured by PTT. Both converge on factor X in the common pathway. Thrombin converts fibrinogen to fibrin. Factor XIII cross-links it into a mesh. When clinical medicine give you an isolated PT elevation, think extrinsic (factor VII, warfarin). Isolated PTT elevation = intrinsic (hemophilia A/B, heparin).
What is Hemostasis?
Hemostasis is the creation of a blood clot following injury to a blood vessel. It's your body's elegant damage control system.
The process happens in three major steps:
- Vasoconstriction → vessel contracts to minimize bleeding
- Platelet Plug Formation → platelets rush to seal the breach (primary hemostasis)
- Fibrin Clot Formation → protein factors create a stable, permanent clot (secondary hemostasis)
Hemostasis breaks into two questions on every vignette. (1) Primary or secondary? Primary = vessel + platelets (immediate plug, seconds). Secondary = clotting cascade (fibrin mesh, minutes). (2) If broken, where? Primary defect → mucocutaneous bleeds (epistaxis, gums, petechiae, menorrhagia). Secondary defect → deep bleeds (hemarthrosis, intramuscular, intracranial). The pattern of bleeding tells you which arm is broken before you order a single lab.
Wound Healing Timeline
Click each step to reveal what happens:
The First Response: Smooth muscle cells in the endothelium contract reflexively when injured.
Trigger: Local sympathetic contraction
Main Job: Stop blood loss by reducing vessel diameter
Reality check: This is your body's immediate "pinch" response. It's fast but temporary→it can't hold on its own.
Platelets Step In: Circulating platelets sense the exposed collagen on the vessel wall and activate.
Main Participant: Platelet cells (thrombocytes)
Trigger: Exposure of subendothelial collagen
Main Job: Create a temporary physical plug (like stuffing a hole with cotton)
Timeline: Happens in seconds. This is the initial seal.
The Permanent Fix: Clotting factors cascade to form fibrin, creating a stable, reinforced clot.
Main Participant: Protein clotting factors (II, V, VII, VIII, IX, X, XI, XII)
Trigger: Exposure of tissue factor and collagen surface
Main Job: Create a stable, reinforced clot that won't wash away
Timeline: Takes minutes. This is the permanent solution.
Memory Hooks
Tap each hook to unlock the board logic behind it.
Platelets (Thrombocytes)
The Quick Story: Platelets are the first responders. They form the temporary plug.
Key Facts:
- First cells to respond in primary hemostasis
- Origin: Megakaryocytes in bone marrow
- Stimulated by: Thrombopoietin (TPO)
- Lifespan: 4-7 days in circulation
- Normal count: 150,000-350,000/microL
- Responsible for: Bleeding from skin and mucosal surfaces
Platelet Count Classifications:
- 150,000-350,000 = Normal
- >350,000 = Thrombocytosis (too many)
- <150,000 = Thrombocytopenia (too few, bleeding risk)
Platelet count threshold map: >50,000 = generally safe for most procedures and minor trauma. 20,000·50,000 = post-trauma bleeding risk; hold elective surgery. <20,000 = spontaneous mucocutaneous bleeding (gums, nose, petechiae). <10,000 = spontaneous CNS / GI bleeding risk · transfuse. clinical medicine love the <10K threshold for "give platelets even if asymptomatic." ITP usually presents in this range with isolated thrombocytopenia and normal coag.
Bleeding Manifestations: Recognize the Pattern
Match the bleeding pattern to its definition. Click each card to reveal the answer:
Tap a zone on the body. Surface = primary hemostasis (platelets). Deep = secondary hemostasis (factors).
Tap the red skin zones or blue deep zones to learn which hemostatic defect causes bleeding at each location.
Primary Hemostasis (Platelet Plug)
| Aspect | Primary Hemostasis |
|---|---|
| Main Participant | Platelets |
| Trigger | Subendothelial collagen exposure |
| Type of Clot | Temporary, physical plug |
| Timeline | Seconds |
| Test (board) | Bleeding time, platelet count |
| Problems → Bleeding From | Skin & mucous membranes (petechiae, purpura) |
Secondary Hemostasis (Fibrin Clot)
| Aspect | Secondary Hemostasis |
|---|---|
| Main Participant | Clotting factors (proteins) |
| Trigger | Tissue factor + collagen exposure |
| Type of Clot | Stable, reinforced fibrin clot |
| Timeline | Minutes |
| Test (board) | PT, aPTT, bleeding time, thrombin time |
| Problems → Bleeding From | Deep tissues, joints, muscles (hematomas) |
Decision Tree: Where Are the Clots?
A patient is forming clots. Where are they forming? Challenge yourself before looking at the answer.
Board Pearl: Stasis = venous. Endothelial injury = arterial. Factor V Leiden = genetic venous.
The Lineup
Tap to flip.
VWD Type 1
- Defect: Low vWF quantity (quantitative)
- Inheritance: Autosomal dominant
- Labs: Bleeding time up, aPTT up, PT normal
- Treatment: DDAVP for mild; vWF concentrate for severe
- Board pearl: Most common inherited bleeding disorder overall
VWD Type 2
- 2A: No platelet binding (large multimers absent)
- 2B: Gain of function, platelet binding too strong, thrombocytopenia
- 2M: Reduced platelet binding but normal multimers; normal RIPA
- 2N: Can't bind Factor VIII; mimics Hemophilia A
VWD Type 3
- Defect: Near-complete absence of vWF
- Inheritance: Autosomal recessive
- Severity: Most severe form
- Treatment: vWF concentrate (not DDAVP; no vWF to release)
- Board pearl: Factor VIII also drops because vWF carries it
Hemophilia A
- Factor: VIII deficiency
- Inheritance: X-linked recessive
- Labs: aPTT up, PT normal, normal bleeding time
- Bleeding: Hemarthrosis, deep muscle bleeds
- Treatment: Recombinant FVIII; DDAVP for mild cases
Hemophilia B
- Factor: IX deficiency
- Inheritance: X-linked recessive
- Labs: aPTT up, PT normal (identical to Hemophilia A on labs)
- Distinguish: Factor assay (IX vs VIII activity)
- Treatment: Recombinant FIX concentrate
Bernard-Soulier
- Defect: GpIb (platelet receptor for vWF) absent or dysfunctional
- Inheritance: Autosomal recessive
- Hallmark: Giant platelets on smear
- Labs: Prolonged bleeding time, low platelet count
- Board pearl: Platelet adhesion (not aggregation) is broken
Glanzmann Thrombasthenia
- Defect: GpIIb/IIIa (fibrinogen receptor) absent
- Inheritance: Autosomal recessive
- Labs: Normal platelet count, prolonged bleeding time, NO aggregation
- Board pearl: Aggregation is broken (compare: Bernard-Soulier breaks adhesion)
ITP
- Mechanism: IgG antibodies against GpIIb/IIIa; spleen destroys coated platelets
- Labs: Low platelets, normal PT and aPTT
- Findings: Petechiae, mucosal bleeding, no systemic illness
- Treatment: Steroids first, then IVIG; splenectomy for refractory
The bleeding lineup boils down to four buckets and four labs: (1) Platelet count · low → ITP, TTP, HIT, DIC, drug, sequestration. (2) PT (extrinsic, 7) · isolated up → warfarin, early liver, Factor VII. (3) PTT (intrinsic, 8/9/11/12) · isolated up → hemophilia A/B, vWD, heparin. (4) Both up · → DIC, severe liver, vitamin K deficiency (2,7,9,10), Factor X. Add a mixing study: corrects = factor deficiency, doesn't correct = inhibitor. Four labs, every bleeding stem you'll see.
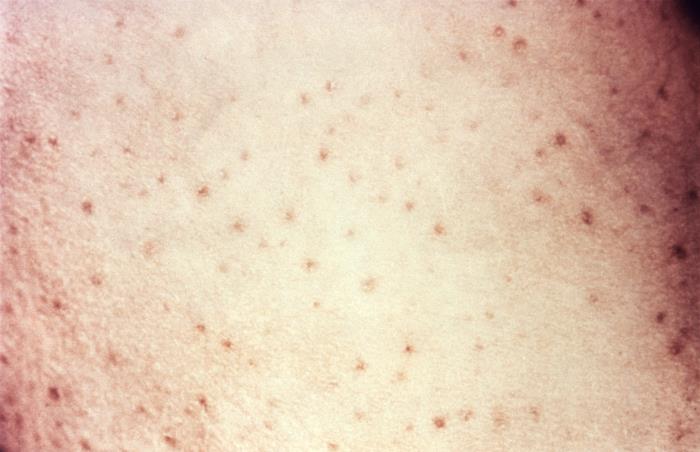
Clinical Photos
Real findings from bleeding disorders.


Work through the algorithm. Each answer reveals the next step. Challenge yourself before tapping.
The algorithm is always the same. Step 1: platelet count + PT + PTT. Step 2: which is abnormal? Isolated PT = extrinsic (VII). Isolated PTT = intrinsic (8, 9, 11, 12) then mixing study. Both = common pathway or global (DIC, liver, vitamin K). Normal coags with bleeding = platelet disorder. Every clinical medicine question gives you exactly enough labs to enter this tree. Follow it and you won't miss.
Tap a clinical feature, then tap the disorder bucket it belongs to. Each feature maps to exactly one disorder.
Four low-platelet disorders, four different mechanisms. ITP = autoimmune destruction (anti-GpIIb/IIIa), isolated low platelets, nothing else abnormal. TTP = ADAMTS13 deficiency, microthrombi shred RBCs (schistocytes), pentad. DIC = cascade fires everywhere, consumes everything (platelets + factors + fibrinogen), always triggered by something (sepsis, trauma, malignancy). HIT = anti-PF4 antibodies from heparin, causes clotting not bleeding. If the stem says "heparin 7 days ago + new clot," stop reading and pick HIT.
Decision Tree: Bleeding Disorder Workup
The workup tree is your safety net on every "what test next?" question. Step 1: name the bleeding type (mucocutaneous vs deep). Step 2: platelet count + PT + PTT (always all three first). Step 3: targeted second-line · bleeding time / PFA-100 (vWD, qualitative platelet defect), peripheral smear (TTP schistocytes, DIC, leukemia), mixing study (factor deficiency vs inhibitor), specific factor levels (8, 9, vWF antigen). If you skip the algorithm and go straight to "send a vWF panel," you'll miss the easy DIC or warfarin answer.
Board Walkthrough
25 original clinical vignettes. One at a time. Right-click or long-press to cross out. Double-tap to highlight.