Board PearlNSAID blocks COX → no prostaglandins → no pain. This is the mechanism you will be tested on.
🦻Primary dysmenorrhea requires a NORMAL pelvic exam. Any structural pathology (endometriosis, fibroids, adenomyosis, PID) moves you to secondary dysmenorrhea. The exam is your gating question.
Board Challenge
Before You Read Any Further
One vignette. Two questions. See where you stand.
Gate Challenge · Step 1 of 2
What is the most likely diagnosis?
A 17-year-old presents with monthly crampy lower abdominal pain that begins about 12 hours before her period and lasts 2 to 3 days. She reports associated nausea, loose stools, and a headache each cycle. Her periods are regular. Pelvic exam is entirely normal. She takes ibuprofen and gets significant relief.
PID requires ascending infection: fever, cervical motion tenderness, adnexal tenderness, purulent discharge. A normal exam with cyclic, NSAID-responsive pain is not PID.
Endometritis is a uterine infection, typically post-procedure or postpartum, presenting with fever and constant (not cyclic) uterine tenderness. This patient has no fever, no instrument history, and a perfectly normal exam.
Correct. Cyclic lower abdominal pain starting just before menses, GI/systemic symptoms, normal exam, and NSAID response = classic primary dysmenorrhea. The normal exam is the gate: no pathology found means the pain source is prostaglandins, not structure.
PMS involves mood, bloating, and irritability in the late luteal phase, resolving with menses onset. This patient's pain is worst WITH menses, not before it, and her symptoms are physical rather than behavioral. PMS does not cause the GI storm she describes.
Gate Challenge · Step 2 of 2
What is the PRIMARY mechanism driving her nausea and loose stools with each cycle?
Normal flora does not ascend in sufficient quantity to cause toxin-mediated GI illness in cyclic, predictable fashion. This is a cyclic prostaglandin effect, not an infection. The normal exam and NSAID response rule out any infectious mechanism.
Progesterone falls at the end of every luteal phase, which is normal menses physiology. That fall triggers the shed, but progesterone deficiency itself does not explain the nausea and diarrhea. The GI symptoms track with prostaglandin production, not progesterone level.
Exactly right. Prostaglandins released by the shedding endometrium do not stay local. They enter the bloodstream and hit smooth muscle everywhere: uterine muscle contracts (cramps), GI smooth muscle contracts (nausea, vomiting, diarrhea), and central vasculature is affected (headache, fatigue). This systemic PG effect is the reason NSAID treatment is first-line: block prostaglandin synthesis and the whole cascade shuts down.
Vagal stimulation from pain can cause nausea, and that does contribute. But the mechanism being tested here is the direct effect of prostaglandins on gut smooth muscle, which explains the diarrhea component that vagal pain does not. Board questions want the molecular mechanism, not the pain reflex.
1 / 5
The Lineup
Primary vs Secondary
Five diagnoses. One has no structural pathology. The others all have something wrong in the pelvis. Tap each card to reveal the clinical picture and the board kill.
🦻
Primary Dysmenorrhea
PGF2-ALPHA DRIVEN
Normal Pelvis
No pathology. Pure prostaglandin storm. Starts within 6-12 months of menarche in young patients.
tap to reveal the board picture →
Primary Dysmenorrhea
Onset: within 6-12 months of menarche (young, often teenage)
Character: crampy lower abdominal pain, D1-2 of menses
Trigger: instrument history (IUD, D&C, delivery, hysteroscopy)
Onset: CONSTANT pain, NOT tied to menstrual cycle
Fever: YES (primary dysmenorrhea never has fever)
Exam: uterine tenderness on bimanual + purulent discharge
No fever, no discharge, normal exam, cyclic = never endometritis
Board kill: Endometritis is an INFECTION. Primary dysmenorrhea is hormonal. If there is fever, the diagnosis is not primary dysmenorrhea.
🔎The one question that splits the whole differential: What does the pelvic exam show? Normal = primary. Tender uterus or cervix = infection. Nodularity or adnexal mass = structural secondary cause. Never skip the exam in your vignette analysis.
2 / 5
The Kills
Kill the Wrong Answers
These are the choices boards put in front of you. Know why each one dies.
KILL #1: Endometritis. Students pick this because "endometrium" is in the name. Here is why it dies: Endometritis is an infection. Bacteria invaded the uterine cavity, usually after a procedure. You get fever, constant (not cyclic) pain, uterine tenderness, and purulent discharge. Primary dysmenorrhea has NONE of those things. The pelvis is normal. There is no fever. The pain follows the menstrual cycle. If there is a fever on the stem, you are not in primary dysmenorrhea. Full stop.
KILL #2: Pelvic Inflammatory Disease. PID is ascending infection (Gonorrhea, Chlamydia) reaching the uterus, fallopian tubes, and ovaries. The exam is never normal: you get cervical motion tenderness (Chandelier sign), bilateral adnexal tenderness, and fever. The pain is not tied to menstrual cycling; it is acute and constant. A teen with cyclic cramps, normal bimanual, and NSAID relief cannot have PID. No cervical motion tenderness = no PID.
KILL #3: Premenstrual Syndrome. PMS involves mood changes (irritability, depression, anxiety), bloating, breast tenderness, and fatigue during the late luteal phase (days 14-28), with relief when menses begins. Primary dysmenorrhea is the opposite: the pain starts with menses and the luteal phase is symptom-free. The patient's worst day in PMS is just before her period. The patient's worst day in primary dysmenorrhea is the first day of her period. Different timing. PMS improves when menses starts; primary dysmenorrhea BEGINS when menses starts.
KILL #4: Secondary Dysmenorrhea (the sneaky one). Secondary dysmenorrhea looks identical to primary except for the history and exam. Signals that should shift you: onset years after menarche, pain that is WORSENING progressively, any abnormality on pelvic exam (nodularity, tenderness, adnexal mass), dyspareunia, or infertility. A board stem will make the case look like primary at first glance, then bury one detail (progressive worsening over 4 years, dyspareunia) that makes it secondary. Primary dysmenorrhea is stable and unchanged since menarche. Secondary is new-onset or progressive.
Memory Hooks
Locks That Stick
Tap each card to reveal the teaching hook.
Memory Hook 1
PG = Pain Generator
Prostaglandins are the ONLY reason primary dysmenorrhea exists. No prostaglandins = no cramps. This is why NSAIDs work: they block COX enzymes, which cuts prostaglandin synthesis at the source. Think of PGF2-alpha as the pain's fuel line, and NSAIDs as the cut valve.
tap to reveal
Memory Hook 2
Normal Exam = Primary Rule
The pelvic exam is the gating question in every dysmenorrhea stem. If the exam is completely normal, structural causes are out. You are dealing with a prostaglandin problem in a healthy pelvis. Any finding on the exam (tenderness, nodularity, mass) pulls you into secondary territory immediately. Abnormal exam means something is there causing the pain.
tap to reveal
Memory Hook 3
Endometritis vs Endometriosis: Infection vs Estrogen
Endometritis ends in "-itis" = inflammation/infection. Bacteria. Fever. Constant uterine tenderness. Post-procedure history. Endometriosis ends in "-osis" = a process (ectopic endometrial growth). Estrogen-driven. Cyclic. Progressive. Dyspareunia. No fever. Two completely different diseases hiding behind similar-sounding names. The board knows you confuse them.
tap to reveal
Memory Hook 4
Primary Starts With Menarche, Secondary Starts Later
Primary dysmenorrhea begins within 6-12 months of the first period and stays stable. Secondary dysmenorrhea either starts later (new-onset pain after years of pain-free cycles) or gets progressively worse after years of mild symptoms. Timing is everything. A 30-year-old whose dysmenorrhea started 2 years ago is not primary. A 16-year-old with pain since her first cycle probably is.
tap to reveal
Memory Hook 5
The Systemic Storm: GI + Head = PG Overflow
The nausea, vomiting, diarrhea, and headache of primary dysmenorrhea are board bait. Students see GI symptoms and jump to a GI diagnosis. But these symptoms are caused by prostaglandins entering systemic circulation and hitting every smooth-muscle-containing organ. The GI symptoms start with the period, not randomly. That timing is the clue. Systemic PG = GI storm every cycle. Not food. Not a GI condition.
tap to reveal
Memory Hook 6
NSAID First, OCP Second
First-line treatment is NSAIDs started 1-2 days before menses. They block COX-1 and COX-2, reducing prostaglandin synthesis in the endometrium. If NSAIDs fail or are contraindicated, second-line is combined hormonal contraceptives (OCPs), which suppress ovulation and reduce endometrial proliferation, cutting the amount of prostaglandin-secreting tissue. GnRH agonists and surgery are reserved for secondary causes or endometriosis.
tap to reveal
3 / 5
Anatomy
Know the Architecture
The structures involved. Tap any image to enlarge.
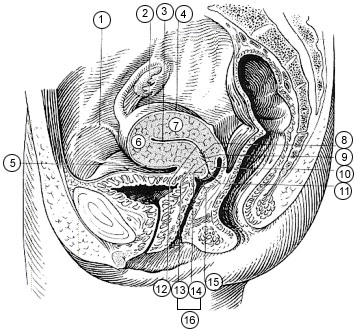
📷 Female Reproductive System · Anatomy Diagram
📷 Uterus & Cervix · Cross-Section Anatomy
📷 Female Pelvis · Pelvic Anatomy Overview
Female Reproductive SystemThe site of primary dysmenorrhea is the uterine endometrium. At menses, the endometrium sheds and releases PGF2-alpha. That prostaglandin causes uterine smooth muscle contraction (cramps), vasoconstriction (ischemia = more pain), and enters systemic circulation to affect the GI tract and brain.Wikimedia Commons, public domain
Uterus & Cervix AnatomyThe endometrial lining (inner layer of the uterine body) is where primary dysmenorrhea originates. Normal structural anatomy here is required for the diagnosis: no fibroids, no adenomyosis, no polyps. The myometrium (muscle wall) contracts forcefully under prostaglandin stimulation, causing the characteristic crampy pain.Wikimedia Commons, public domain
Female Pelvis OverviewThe normal pelvic exam in primary dysmenorrhea: no adnexal tenderness, no cervical motion tenderness, no uterosacral nodularity, no adnexal masses. The physical examination is your single most important discriminator. Any abnormality here pushes you toward secondary causes (endometriosis, adenomyosis, PID).Wikimedia Commons, public domain
Board Trap · The Anatomy Clue: When a stem describes a normal pelvic exam in detail ("uterus midline, normal size, no adnexal tenderness, no cervical motion tenderness"), the examiners are telling you there is no structural pathology. That detail is not filler. It is the elimination key for every secondary cause.
Clinical Decision Tree
Cyclic Pelvic Pain Workup
Three questions. Follow the logic to the diagnosis and treatment.
Workup Tree · Step 1 of 3
A patient presents with painful periods. What is the MOST critical first assessment?
Ultrasound has a role in ruling out structural pathology, but it is not the first step. A pelvic exam is always done first and guides what imaging, if any, is needed. An exam costs nothing and takes two minutes. A normal exam essentially rules out the major structural secondary causes.
Yes. The pelvic exam is the gate. Normal exam = primary dysmenorrhea territory. Any finding (tenderness, nodularity, cervical motion tenderness, adnexal mass) opens the secondary dysmenorrhea differential. Exam first, imaging after, based on what you find.
Empirically starting antibiotics without exam findings is overtreatment and diagnostic error. PID requires specific exam criteria (cervical motion tenderness, uterine tenderness, adnexal tenderness). Cyclic pain with a normal exam does not meet PID criteria.
Contraceptive history is relevant later (OCPs are second-line treatment and change the differential), but it does not come first. The exam determines whether you are dealing with a structural or hormonal problem before you consider treatment options.
Workup Tree · Step 2 of 3
Pelvic exam is NORMAL. The patient is 16, menstruating for 14 months, pain starts day 1 of menses, associated nausea. What is the diagnosis?
Secondary dysmenorrhea requires a structural cause. A normal exam in a 16-year-old who has had pain since near menarche is the definition of primary. Endometriosis can occur in teenagers but would not present with a completely normal exam at this stage.
Correct. All four criteria met: onset within 6-12 months of menarche, crampy pain with menses, systemic prostaglandin symptoms (nausea), and a normal pelvic exam. Primary dysmenorrhea. Go to treatment.
PID requires exam findings (cervical motion tenderness, adnexal tenderness, uterine tenderness) plus typically fever. Normal exam in a teenager with cyclic pain is not PID. Treating a primary dysmenorrhea patient with antibiotics is both unnecessary and diagnostic overreach.
Adenomyosis presents in parous women in their 40s with an enlarged, boggy, tender uterus and heavy periods. A 16-year-old with a normal exam does not have adenomyosis.
Workup Tree · Step 3 of 3
Primary dysmenorrhea confirmed. What is the appropriate first-line treatment?
Laparoscopy is the definitive diagnostic tool for endometriosis, not primary dysmenorrhea. Surgery on a patient with a normal exam and a classic primary dysmenorrhea picture is not indicated. Try NSAIDs first.
First-line. NSAIDs (ibuprofen, naproxen) started 1-2 days before menses onset prevent prostaglandin buildup before it starts. By blocking COX enzymes, you cut PGF2-alpha synthesis in the endometrium. If NSAIDs fail, combined OCPs are second-line. Surgery is never first-line here.
GnRH agonists suppress the HPG axis, reducing estrogen and inducing a pseudomenopause state. They are reserved for endometriosis treatment or severe refractory cases after diagnosis is confirmed. Way too aggressive for first-line primary dysmenorrhea management.
Opioids are not used for primary dysmenorrhea. They address pain without targeting the mechanism (prostaglandins). NSAIDs fix the mechanism AND the pain. Using opioids first is pharmacologically backwards.
4 / 5
Board Walkthrough
See If It Stuck
Eight original vignettes. Tap an answer. Expand wrong choices to read the kill explanation.
Each vignette is 3rd-order: you need the mechanism, the discriminator, or the clinical context, not just the name.
Board Vignette · 1 of 8
A 17-year-old presents with monthly crampy lower abdominal pain beginning approximately 12 hours before her period and lasting the first 2 days of menses. She reports nausea, vomiting, and loose stools with each episode. Her last menstrual period was 14 months after menarche and her cycles are regular at 28 days. Pelvic examination is completely normal. She takes ibuprofen 600 mg at onset and her pain decreases substantially.
What is the PRIMARY mechanism driving her gastrointestinal symptoms with each menstrual cycle?
ARetrograde uterine compressiontap to expand
Good mechanical instinct, but retrograde compression does not explain nausea and vomiting. Anatomical compression of the colon causes obstructive symptoms or constipation, not the nausea-diarrhea-vomiting triad you see here. Also, this patient has a completely normal pelvic exam, and her symptoms are too consistent and predictable to be mechanical. Mechanical compression does not cause the nausea-vomiting-diarrhea storm of primary dysmenorrhea. Prostaglandins do.
BBacterial toxin releasetap to expand
Good instinct to think infection when you see GI symptoms, but this patient has no fever, no abnormal discharge, and a normal pelvic exam. Bacterial toxin-mediated GI illness is not cyclic and predictable to the day of menses. Bacterial infections do not cause consistent, ibuprofen-responsive GI symptoms synchronized with the menstrual cycle. No fever, no discharge, normal exam, NSAID-responsive = prostaglandins, not bacteria.
CPGF2-alpha stimulating GI smooth muscleCORRECT
This is the systemic prostaglandin effect. When the endometrium sheds, it releases PGF2-alpha into local circulation. PGF2-alpha does not stay in the uterus. It enters systemic circulation and hits every smooth-muscle-containing organ: uterine smooth muscle contracts causing cramps, GI smooth muscle contracts causing nausea, vomiting, and diarrhea, and central vasculature is affected causing headache and fatigue. NSAIDs cut this entire cascade by blocking COX enzymes upstream. Systemic PGF2-alpha = the full-body storm of primary dysmenorrhea, not just cramps.
From a mechanism standpoint, the GI symptoms are as prostaglandin-driven as the cramps. The diarrhea, in particular, is a classic board clue for primary dysmenorrhea. Boards will put GI symptoms in the stem to see if you trace them back to the mechanism.
DProgesterone withdrawal triggering dysmotilitytap to expand
Progesterone does fall at the end of the luteal phase, and that withdrawal triggers menstrual shedding. But progesterone withdrawal itself does not cause nausea, vomiting, and diarrhea in a predictable, NSAID-reversible pattern. The symptom generator is what the endometrium releases when it sheds: prostaglandins. Progesterone sets the stage; prostaglandins cause the show. Progesterone withdrawal triggers the shed. PGF2-alpha causes the symptoms. These are two different steps in the same pathway.
Board Vignette · 2 of 8
A 29-year-old nulliparous woman has had progressively worsening pelvic pain with menses over the past 4 years. The pain now starts 2 days before her period and has increased from mild to severe over time. She also reports deep dyspareunia and has been unable to conceive after 18 months of unprotected intercourse. Bimanual exam reveals nodularity palpable along the left uterosacral ligament.
Which feature MOST clearly distinguishes this case from primary dysmenorrhea?
ASeverity of paintap to expand
Pain severity alone does not separate primary from secondary. Primary dysmenorrhea can be severe (8-9/10). Endometriosis can be mild. The diagnosis is determined by mechanism and findings, not the number on the pain scale. Pain intensity does not discriminate primary from secondary dysmenorrhea.
BStructural pelvic pathologyCORRECT
Uterosacral nodularity is an exam finding. It represents ectopic endometrial deposits on the uterosacral ligaments, a hallmark of endometriosis. Primary dysmenorrhea NEVER has exam findings. By definition, the pelvis is structurally normal. The moment you have a palpable abnormality, you have left primary dysmenorrhea and entered secondary territory. The progressive course, dyspareunia, infertility, and this nodularity all point to endometriosis. Any pelvic exam finding eliminates primary dysmenorrhea. Structural pathology = secondary. Always.
The dyspareunia clue is also key: endometriosis causes deep dyspareunia because ectopic deposits are on the uterosacral ligaments, posterior cul-de-sac, and rectovaginal septum, all of which are under tension during intercourse. Primary dysmenorrhea does not cause dyspareunia.
CFailure to respond to ibuprofentap to expand
NSAID failure is a RED FLAG for secondary causes but it is not the defining discriminator. Endometriosis also has a prostaglandin component, so it can partially respond to NSAIDs. Also, we do not have information about NSAID response in this case. The exam finding is the hard discriminator. NSAID failure is a clue for secondary causes but not the defining criterion. Exam findings are.
DAge of onsettap to expand
Age of onset is a supporting clue, not the defining discriminator. Primary dysmenorrhea typically starts within 6-12 months of menarche; this patient had pain since her late 20s. That timing suggests secondary causes. But age alone would not be the MOST distinguishing feature compared to an actual abnormal physical exam finding. Age is suggestive but exam findings are definitive.
Board Vignette · 3 of 8
A 16-year-old with a 10-month history of primary dysmenorrhea begins taking ibuprofen 400 mg three times daily starting the day before her expected menses. Her pain decreases from 8/10 to 2/10. She asks how the medication works.
What is the mechanism by which ibuprofen reduces her dysmenorrhea?
ACalcium channel blockade on uterine smooth muscletap to expand
Calcium channel blockers (nifedipine, etc.) do relax smooth muscle, but that is NOT ibuprofen's mechanism. Ibuprofen is a COX inhibitor. It works upstream by stopping prostaglandin production, not downstream by blocking calcium channels. If you confuse these, you will also confuse tocolytics with NSAIDs. Ibuprofen = COX inhibitor. Calcium channel blockers = different class, different target.
BDecreases endometrial thicknesstap to expand
Thinning the endometrium is the mechanism of combined OCPs (second-line) and progestins, not NSAIDs. NSAIDs do not alter endometrial growth or thickness. They work acutely: take them, stop making prostaglandins, feel better. No chronic tissue remodeling involved. Endometrial thinning = hormonal contraceptives. Prostaglandin reduction = NSAIDs. Different tools, different targets.
This is the mechanism you will be asked about. Arachidonic acid is converted to prostaglandins via cyclooxygenase (COX) enzymes. NSAIDs (ibuprofen, naproxen, mefenamic acid) inhibit COX-1 and COX-2. With COX blocked, arachidonic acid cannot become PGF2-alpha. Less PGF2-alpha means less uterine contraction, less vasoconstriction, less ischemia, and less systemic effect (less nausea, less GI upset). The medication works upstream at synthesis, not at the receptor. Starting it before menses prevents the prostaglandin buildup entirely. NSAIDs block COX → no prostaglandins → no pain cascade. This is why they work.
Starting NSAIDs 24-48 hours BEFORE expected menses onset is more effective than waiting until pain starts, because prostaglandins are already being produced in the late luteal phase before the period arrives.
DBlocks prostaglandin receptors on uterine smooth muscletap to expand
Close, but mechanistically wrong. Prostaglandin receptor blockade is the mechanism of specific drugs like misoprostol antagonists. NSAIDs work upstream: they block the enzyme (COX) that MAKES prostaglandins, so the prostaglandins never get produced. Receptor blockers would still allow prostaglandins to be made; they just prevent binding. NSAIDs prevent the synthesis. NSAIDs stop prostaglandin synthesis. Receptor blockers stop prostaglandin binding. NSAIDs are upstream at the enzyme.
Board Vignette · 4 of 8
A 31-year-old nulliparous woman presents with new-onset cyclic pelvic pain that began 9 months ago. The pain starts 2-3 days before her period and persists throughout menses. She also notes deep dyspareunia that has become worse over the same period. Her periods have always been regular. Pelvic exam: uterus normal in size and mobility; tenderness elicited on palpation of the right uterosacral ligament; no adnexal masses.
What is the most appropriate next step in her management?
AReassure as primary dysmenorrheatap to expand
You cannot call this primary dysmenorrhea. Primary requires a NORMAL pelvic exam. This patient has uterosacral ligament tenderness, which is a physical exam finding. Combine that with new-onset pain at age 31, progressive course, and deep dyspareunia, and you have a secondary cause until proven otherwise. Reassuring as primary would mean missing endometriosis. Abnormal pelvic exam = not primary dysmenorrhea. Period.
BAntibiotics for endometritistap to expand
Endometritis has a constant, non-cyclic presentation with fever and purulent discharge, usually following a uterine procedure. This patient has no fever, no discharge, no instrument history, and a pain pattern that is cyclic and progressive. Antibiotics would be actively wrong here. The presentation is endometriosis, not endometritis. Cyclic, progressive, dyspareunia, uterosacral tenderness = endometriosis. Not an infection.
CDiagnostic laparoscopyCORRECT
Laparoscopy is the definitive diagnostic tool for endometriosis. Pelvic exam and ultrasound can raise suspicion but cannot rule out endometriosis in a patient with this constellation: new-onset secondary dysmenorrhea in a nulliparous woman in her 30s, progressive course, dyspareunia, and uterosacral ligament tenderness. You need direct visualization of peritoneal implants. Once confirmed, you also get the opportunity for surgical treatment (excision or ablation). Suspected endometriosis + desire to confirm + possible surgical treatment = diagnostic laparoscopy.
Note: ultrasound can detect endometriomas (ovarian chocolate cysts) but misses peritoneal implants. CA-125 is non-specific. The only way to definitively diagnose endometriosis is visual inspection with biopsy at laparoscopy.
DEmpiric GnRH agonisttap to expand
GnRH agonists are a treatment for endometriosis, but empirically prescribing them without diagnosis is incorrect. They cause menopausal side effects (hot flashes, bone loss) and do not provide a definitive diagnosis. Also, response to GnRH agonist does not confirm endometriosis (primary dysmenorrhea would also respond). You need the diagnosis first. GnRH agonists treat endometriosis; they do not diagnose it. Confirm with laparoscopy first.
Board Vignette · 5 of 8
A 24-year-old woman presents to the emergency department with pelvic pain. She had an IUD placed 3 weeks ago. The pain is constant, not related to her menstrual cycle. Temperature is 38.8 degrees C. Bimanual exam: uterus tender to palpation; mucopurulent cervical discharge. WBC 15,800 with 88% polymorphonuclear cells. She is not currently menstruating.
What is the most likely diagnosis, and what SINGLE feature most clearly distinguishes it from primary dysmenorrhea?
APrimary dysmenorrheatap to expand
This patient has fever, constant (not cyclic) pain, uterine tenderness, purulent discharge, and leukocytosis after a uterine procedure. That is the opposite of primary dysmenorrhea. Primary dysmenorrhea has no fever, follows the menstrual cycle, and has a completely normal exam. Instrument procedures can transiently worsen primary dysmenorrhea but they do not cause infectious endometritis findings. Fever + purulent discharge + uterine tenderness after instrument = endometritis. Not primary dysmenorrhea.
BEndometritisCORRECT
This is the endometritis trap case. IUD placement 3 weeks ago introduces bacteria into the uterine cavity. The result: ascending infection of the endometrium. The key discriminators from primary dysmenorrhea are: FEVER (primary dysmenorrhea never has fever), CONSTANT pain (not cyclic), UTERINE TENDERNESS on exam (primary dysmenorrhea: normal exam), PURULENT DISCHARGE (primary dysmenorrhea: none), and LEUKOCYTOSIS. Every one of those features rules out primary dysmenorrhea. Endometritis = infection. Primary dysmenorrhea = hormonal. That is the board discriminator: if there is fever, the diagnosis is not primary dysmenorrhea.
Endometritis vs Endometriosis is a separate killer: endometritis is acute infection (post-procedure, postpartum) while endometriosis is chronic, estrogen-driven ectopic growth. Both are different from primary dysmenorrhea. Three different diagnoses, three different stories.
CSecondary dysmenorrhea from IUD mechanical irritationtap to expand
IUDs (especially copper IUDs) can worsen dysmenorrhea due to increased prostaglandin production. But that would be cyclic pain tied to menses without fever. This patient has fever, constant pain unrelated to her cycle, purulent discharge, and leukocytosis. That is infection, not mechanical irritation. Mechanical IUD-related pain also does not cause fever or a purulent discharge. IUD-related dysmenorrhea is cyclic and afebrile. Fever + discharge + constant pain = infection, not mechanics.
DOvarian torsiontap to expand
Ovarian torsion presents with sudden-onset severe unilateral pelvic pain, often with nausea and vomiting, and may be associated with an adnexal mass (the weight that causes torsion). It does not cause fever or purulent discharge. The uterine tenderness in this case is the site of infection, not torsion. An IUD would not cause torsion. Ovarian torsion = sudden unilateral + adnexal mass. No fever, no discharge. Wrong pattern entirely.
Board Vignette · 6 of 8
A 17-year-old has been using ibuprofen for primary dysmenorrhea with 60% improvement in pain. She takes it at the usual dose for 3 cycles. She asks her physician whether a combined oral contraceptive pill could offer additional benefit.
What is the mechanism by which combined OCPs reduce dysmenorrhea severity?
AProstaglandin receptor blockade (like NSAIDs)tap to expand
NSAIDs block COX enzymes. They do not block prostaglandin receptors. OCPs do neither. OCPs work hormonally: they suppress the HPG axis, prevent ovulation, and thin the endometrium. These are completely different mechanisms from NSAIDs. OCPs = hormonal suppression of endometrium. NSAIDs = enzyme inhibition. Neither blocks prostaglandin receptors.
Combined OCPs contain estrogen and progestin. They suppress the HPG axis (lowering LH and FSH), preventing ovulation. The progestin component thins the endometrium. Less endometrial tissue = less tissue available to shed = less prostaglandin-producing endometrium = fewer prostaglandins released. Thinner endometrium also means a lighter, shorter, less painful period. OCPs do not block prostaglandins directly; they reduce the amount of endometrium that can produce them. OCPs thin the endometrium = less prostaglandin-secreting tissue = less PGF2-alpha = less pain. Indirect mechanism.
CDirect COX-2 inhibition (like NSAIDs)tap to expand
OCPs are not COX inhibitors. They are hormonal agents. COX-2 inhibition is the mechanism of celecoxib (a selective NSAID), not ethinyl estradiol or levonorgestrel. Confusing these mechanisms would lead to prescribing the wrong drug class. COX-2 inhibition = NSAIDs. OCPs work through hormonal endometrial suppression, not enzyme inhibition.
DIncreased endorphin productiontap to expand
Exercise increases endorphin production and can modestly help with dysmenorrhea, but this is not the mechanism of combined OCPs. Hormonal contraceptives work on the HPG axis and endometrial tissue, not on central pain modulation via endorphin release. Endorphins are for exercise-induced pain relief. OCPs act on the endometrium, not the pain perception pathway.
Board Vignette · 7 of 8
A medical student is reviewing four patients with cyclic pelvic pain and is asked to identify which patient CANNOT have primary dysmenorrhea based on the available clinical information alone.
Patient A: 16-year-old, onset 8 months after menarche, pain starts D1 of period, normal bimanual exam, NSAID-responsive.
Patient B: 28-year-old, new-onset pain 1 year ago, progressive worsening, pain persists between cycles, fixed retroverted uterus and restricted adnexal mobility.
Patient C: 19-year-old, cyclic pain since age 14, nausea and headache with each period, normal pelvic exam, no dyspareunia.
Patient D: 22-year-old, cyclic pain, partial NSAID response, normal pelvic exam, no systemic symptoms.
Which patient CANNOT have primary dysmenorrhea?
APatient Atap to expand
Patient A is the textbook primary dysmenorrhea case: onset within 12 months of menarche, cyclic D1 pain, normal exam, NSAID response. This patient CAN have primary dysmenorrhea. Nothing here excludes it. Patient A fits primary dysmenorrhea criteria precisely.
BPatient BCORRECT
Patient B has a fixed retroverted uterus and restricted adnexal mobility on exam. These are physical exam findings. Primary dysmenorrhea requires a completely normal pelvic exam by definition. A fixed, immobile uterus indicates adhesions or infiltrating pathology, most likely endometriosis with posterior cul-de-sac involvement. Add new-onset pain at 28 with progressive worsening, and this is almost certainly endometriosis. She cannot have primary dysmenorrhea. Fixed uterus + restricted adnexal mobility = structural pathology = secondary dysmenorrhea. Primary requires a normal exam.
CPatient Ctap to expand
Patient C has cyclic pain since age 14, nausea and headache (classic systemic PG symptoms), and a normal pelvic exam. This is a completely consistent primary dysmenorrhea picture. The systemic symptoms are expected, not disqualifying. Patient C fits primary dysmenorrhea: early onset, cyclic, systemic PG symptoms, normal exam.
DPatient Dtap to expand
Patient D has cyclic pain, a normal exam, and partial NSAID response. Partial response to NSAIDs is common in primary dysmenorrhea and does not exclude the diagnosis. The normal exam is the key criterion, and Patient D has it. Partial NSAID response with normal exam is still consistent with primary dysmenorrhea.
Board Vignette · 8 of 8
A 18-year-old with known primary dysmenorrhea since age 15 has tried naproxen and ibuprofen at full doses. Both reduce pain by about 40%, but she continues to miss school 1-2 days per cycle. Pelvic exam is normal. She is sexually active and would consider contraception.
What is the most appropriate next step in her management?
ALaparoscopytap to expand
Laparoscopy is premature here. This patient has a normal pelvic exam, a diagnosis established at age 15, and partial NSAID response, all consistent with primary dysmenorrhea. The appropriate escalation is to the next medical treatment option (OCPs), not surgery. Laparoscopy would be appropriate if OCPs fail AND exam findings or other features suggest endometriosis. Try OCPs before surgery. Normal exam + no secondary features = medical management first.
BCombined oral contraceptive pillsCORRECT
This is the textbook second-line step: NSAIDs (tried, partial response) → combined OCPs. OCPs suppress ovulation and thin the endometrium, reducing prostaglandin-secreting tissue. They also offer contraception, which this patient would welcome. The normal exam confirms there is no secondary pathology driving the inadequate response. Start OCPs. If OCPs fail, then re-examine for endometriosis and consider laparoscopy. NSAIDs fail or partially succeed → combined OCPs. Always. Before laparoscopy or GnRH agonist.
CGnRH agonist (leuprolide)tap to expand
GnRH agonists are used for endometriosis treatment and occasionally refractory primary dysmenorrhea, but they are far too aggressive as the next step here. They cause menopausal symptoms (hot flashes, vaginal dryness) and bone loss with prolonged use. Combined OCPs have a far better side-effect profile and are the appropriate second-line step. GnRH agonists are reserved for when OCPs and conservative management have failed, or when endometriosis is confirmed. GnRH agonist is third- or fourth-line. OCPs come first.
DAmitriptyline for central sensitizationtap to expand
Central sensitization can develop in chronic pelvic pain syndromes, and tricyclics have a role in chronic pain management. But this is not the appropriate next step for a patient with a clear peripheral mechanism (prostaglandins) who has only tried two NSAIDs. Central pain modulation is considered after peripheral causes are adequately treated. Treat the prostaglandin mechanism first. Central sensitization therapies come after peripheral management is optimized.