The Villains
Tap any card to flip it. Front = the drug. Back = mechanism, cast finding, and final rule.
↻ tap to flip
Aminoglycosides
Gentamicin, tobramycin, amikacin
Aminoglycosides
Where: Proximal tubule (PCT)
How: Taken up by megalin receptor into PCT cells, accumulates in lysosomes, triggers cell death from inside
Cast: Muddy brown granular casts
Extras: Ototoxic (hair cell damage) · hypoMg · non-oliguric ATN
Final rule: muddy brown casts + aminoglycoside = toxic ATN. Reversible if caught early.
Cisplatin
Platinum chemo agent
Cisplatin
Where: PCT and DCT
How: Enters tubular cells, crosslinks DNA, triggers apoptosis; also causes oxidative stress
Cast: Muddy brown casts
Extras: HypoMg (tubular Mg wasting), hypoK, ototoxic · prevent with aggressive saline hydration
Final rule: testicular/ovarian cancer chemo + rising Cr + hypoMg = cisplatin ATN.
Contrast Dye
CIN / contrast-induced AKI
Contrast Dye
Where: Medullary tubules (especially TAL)
How: Direct tubular toxicity + renal vasoconstriction (decreased medullary O2 delivery)
Cast: Muddy brown casts
Extras: Cr rises 24-48h post-contrast, peaks at 3-5 days · prevent with IV saline ± NAC
Final rule: CT scan + Cr rise 48h later = contrast nephropathy. Risk up in CKD + DM.
Amphotericin B
Antifungal, IV formulation
Amphotericin B
Where: PCT and DCT membranes
How: Binds cholesterol in tubular cell membranes (like ergosterol in fungi), punches holes, K+ and H+ leak out
Electrolytes: HypoK + type 1 RTA (distal RTA)
Extras: Lipid formulation (AmBisome) is less nephrotoxic
Final rule: amphotericin + hypoK + metabolic acidosis = tubular membrane pore toxicity.
NSAIDs
Aspirin, ibuprofen, naproxen
NSAIDs
Acute: Block PGE2 at afferent arteriole → vasoconstriction → prerenal AKI. Bland sediment, FeNa <1%.
Chronic (months-years): Analgesic nephropathy → papillary necrosis → sloughed papilla can obstruct ureter
Also: Can cause AIN (allergic, reversible)
Final rule: acute NSAID = prerenal (no casts). Chronic NSAID = papillary necrosis. POSTCARDS mnemonic.
Acyclovir / Indinavir
Crystal nephropathy drugs
Crystal Nephropathy
Acyclovir: Needle-shaped crystals in concentrated urine → physical tubular obstruction. Treat with hydration.
Indinavir (HIV): Protease inhibitor crystals in alkaline urine → flank pain, hematuria, crystalluria
Methotrexate: Precipitates at acidic pH → give urinary alkalinization
Final rule: crystals in urine + drug exposure = crystal nephropathy. No muddy brown casts. Hydration is treatment.
Workup Algorithm
Follow the decision tree to identify the type of drug-induced kidney injury.
Drug exposure + rising creatinine
Check urine sediment
Muddy brown granular casts
→ ATN (toxic)
Aminoglycosides, cisplatin, amphotericin B, contrast, myoglobin
Aminoglycosides, cisplatin, amphotericin B, contrast, myoglobin
WBC casts + eosinophiluria
→ AIN (allergic)
Check for fever + rash triad. NSAIDs, methicillin, PPIs, sulfonamides
Check for fever + rash triad. NSAIDs, methicillin, PPIs, sulfonamides
Crystalluria (needle or fan-shaped)
→ Crystal nephropathy
Acyclovir, indinavir, methotrexate. Hydrate aggressively.
Acyclovir, indinavir, methotrexate. Hydrate aggressively.
Bland sediment + FeNa <1% + BUN:Cr >20
→ Prerenal AKI
ACEi / ARBs (efferent dilation), NSAIDs (afferent constriction)
ACEi / ARBs (efferent dilation), NSAIDs (afferent constriction)
ATN confirmed? → Was it reversible?
Yes + preserved basement membrane on biopsy
→ Toxic ATN: tubular cells regenerate from surviving basement membrane. Recovery in 1-3 weeks.
Persistent AIN despite drug removal
→ Consider steroids (prednisone). AIN can progress to CKD if untreated.
Clinical Images
Key histology and clinical concepts. Tap any image to open.
Loading images...
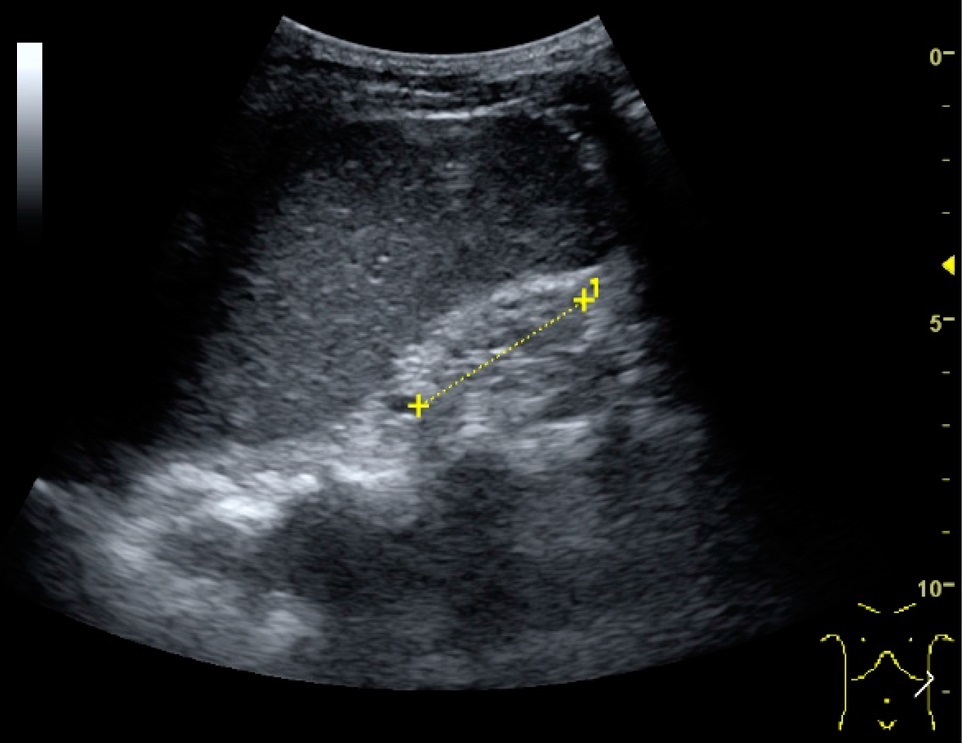
Kidney injury contextChronic kidney disease increases nephrotoxin risk.
Which Drug Is Causing AKI?
Recent new medication + rising creatinine. Follow the culprit.
Recent new medication + rising creatinine?
clinical reference
5 random questions from a pool of 10. All original.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.
