The stress hormone that keeps you alive at 2 AM. HPA axis, three metabolic actions, and the immunosuppression drill that gives you board points.
A medical student is studying for clinical practice at 2 AM when she suddenly receives news that she failed her previous exam. Her heart rate spikes to 110 bpm, her blood glucose rises to 140 mg/dL, and she feels a surge of energy despite being exhausted moments earlier.
Which hormone is primarily responsible for this acute stress response?
THE SOURCE
Where Cortisol Comes From
The HPA axis: three levels, one stress hormone.
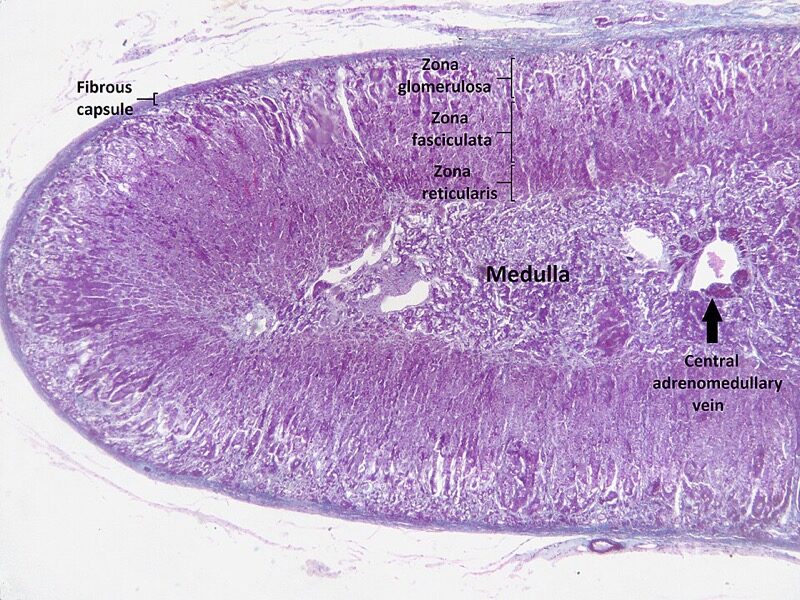
📷 ADRENAL CORTEX: three zones (GFR: salt, sugar, sex) · tap to expand
The HPA Axis
Cortisol production runs on a three-level cascade. Stress and hypoglycemia are the triggers:
CRH hits the anterior pituitary, which releases ACTH (adrenocorticotropic hormone)💡ACTH = "Adrenal Cortex Tell Here." Pituitary to adrenal.
ACTH hits the adrenal cortex, specifically the zona fasciculata, which produces cortisol💡GFR = Glomerulosa (salt), Fasciculata (sugar), Reticularis (sex). Fasciculata = cortisol = the sugar zone.
Cortisol then feeds back to suppress both CRH and ACTH: negative feedbackWhen cortisol levels are high enough, it tells the hypothalamus and pituitary to stop releasing CRH and ACTH. This is why exogenous steroid use can suppress the entire axis, leading to adrenal atrophy.. This is why chronic steroid use causes adrenal suppression: the axis shuts down because exogenous cortisol is doing the job.
Hypothalamus
Senses stress & hypoglycemia
↓
CRH
Anterior Pituitary
Corticotroph cells
↓
ACTH
Adrenal Cortex
Zona Fasciculata
↓
CORTISOL
★Mnemonic: GFR (from outside in) = Glomerulosa, Fasciculata, Reticularis. "Salt, Sugar, Sex" = aldosterone, cortisol, androgens. Cortisol = zona Fasciculata = the Sugar zone.
The Permissive Hormone
Cortisol is called a permissive hormoneA permissive hormone does not directly cause the effect, but without it, other hormones cannot do their jobs. Think of cortisol as the bouncer who keeps the door open: the catecholamines are the ones who walk in and do the work, but without cortisol holding the door, they cannot enter. because it does not act alone. Instead, it enables other hormones to function during stress. The classic example: without cortisol, catecholamines (epinephrine, norepinephrine) cannot properly maintain vascular tone.
This is why patients in adrenal crisis become hypotensive: their catecholamines are there, but cortisol is not present to let them work on blood vessels.
⚠️
Board Trap: Second Messenger
Cortisol is a steroid hormone. Steroid hormones use intracellular receptors that go directly to the nucleus and modify gene transcription. NOT cAMP. NOT tyrosine kinase. If a question asks "what is the mechanism of cortisol action," the answer is intracellular receptor. cAMP is for peptide hormones like ACTH itself, not for cortisol.
THE ACTIONS
What Cortisol Does
Three metabolic actions. Every one of them is a board question. Tap each card to expand.
🍫Gluconeogenesis
Making new glucose from non-carbohydrate sources
tap to expand
What: The liver takes amino acids (from protein breakdown) and glycerol (from fat breakdown) and converts them into brand-new glucose molecules.
Where: Primarily the liver. The liver is the glucose factory.
Why: During stress, the brain and muscles need fuel. Cortisol ensures the liver keeps producing glucose even when dietary intake has stopped.
This is why stressed patients become hyperglycemic
This is why chronic steroid use can cause steroid-induced diabetes
This is why the medical student in the opener had a glucose of 140 mg/dL at 2 AM
★Board connection: Cushing syndrome = chronic cortisol excess = persistent gluconeogenesis = hyperglycemia. The glucose never stops being made.
💪Proteolysis
Breaking down proteins into amino acids
tap to expand
What: Cortisol breaks down skeletal muscle protein into amino acids. Those amino acids get shipped to the liver to feed gluconeogenesis.
Why orthos love steroids (and hate the side effects): Steroids crush inflammation, which is great. But they also break down protein in connective tissue, muscle, and bone. Long-term steroid use leads to:
Muscle wasting (proximal myopathy: thin arms and legs)
Skin thinning (easy bruising, striae)
Osteoporosis (bone matrix is protein)
Poor wound healing (tissue repair needs protein synthesis)
★Board connection: Cushing patients have thin limbs (muscle wasted) but a round face and central obesity. The protein leaves the limbs, the fat goes to the trunk.
🥑Lipolysis
Breaking down fat stores for fuel
tap to expand
What: Cortisol breaks down triglycerides in fat tissue into glycerol and free fatty acids. The glycerol feeds gluconeogenesis. The fatty acids provide direct energy.
The Cushing paradox: Cortisol causes lipolysis in the limbs, but simultaneously promotes central fat redistributionThe mechanism is not fully understood, but visceral fat appears to have more cortisol receptors and insulin sensitivity than peripheral fat. Cortisol plus insulin drives fat deposition centrally while breaking it down peripherally.. This creates the classic Cushing body habitus:
Moon face (fat deposited centrally in the face)
Buffalo hump (dorsocervical fat pad)
Truncal obesity with thin extremities
★Board connection: Central obesity + thin limbs + striae + hyperglycemia = think Cushing syndrome. The body is simultaneously burning and redistributing fat.
📷 CUSHING SYNDROME: central obesity, moon face, thin extremities · tap to expand
THE HPA COMPONENTS
Who Runs the Axis
Three players, one cascade. Tap to flip and learn each player's role.
🧠
The Hypothalamus
CRH release site
tap to flip
CRH: The Starter Gun
Corticotropin-releasing hormone. Released in response to stress and hypoglycemia.
Travels via portal blood to the anterior pituitary. Binds corticotroph cells. Triggers ACTH secretion.
Break it down: stress activates hypothalamus first
🏺
The Anterior Pituitary
ACTH release site
tap to flip
ACTH: The Messenger
Adrenocorticotropic hormone from corticotroph cells. Directly stimulates the adrenal cortex.
Shares precursor (POMC) with MSH: very high ACTH causes hyperpigmentation.
Break it down: high ACTH = skin darkening (ectopic or Addison)
🔥
Zona Fasciculata
Cortisol factory
tap to flip
Cortisol: The Stress Hormone
Made in the zona fasciculata. Steroid hormone: lipophilic, crosses membranes, uses intracellular receptor.
Feeds back negatively to hypothalamus AND pituitary to shut off CRH and ACTH.
Break it down: exogenous steroids suppress both CRH and ACTH
💥
The Feedback Loop
Negative inhibition
tap to flip
Cortisol Suppresses Itself
High cortisol signals the hypothalamus and pituitary to stop. CRH and ACTH drop.
Chronic exogenous steroid use = adrenal axis suppressed for months. Sudden stop = adrenal crisis.
Break it down: never stop chronic steroids abruptly
THE DRILL
IPS: Immunosuppression
"Memorize this one. It will give you a lot of points." Place each chip into the correct letter group.
The IPS Drill
Cortisol suppresses the immune system through three mechanisms. Drag the right actions to each letter.
I= Inhibits Phospholipase A2
What does inhibiting phospholipase A2 prevent?
P= Pacifies Immune Cells
Three things cortisol does to calm the immune army. Place all three.
S= Stabilizes Membranes
Two types of membranes cortisol stabilizes. Place both.
The Complete Answer
When clinical medicine ask "what are the actions of cortisol," the full answer is:
IPS + Lipolysis + Proteolysis + Gluconeogenesis
The IPS mnemonic covers the immunosuppressive actions. The three metabolic actions (lipolysis, proteolysis, gluconeogenesis) cover the metabolic side. Together, that is everything cortisol does.
Treatment Connection: Replacing What is Missing
In congenital adrenal hyperplasiaCAH (21-hydroxylase deficiency) is the most common cause. The enzyme block prevents cortisol and aldosterone synthesis, so all precursors get shunted to androgens. Baby girls virilize. Both sexes salt-waste if the block is severe. (21-hydroxylase deficiency), cortisol and aldosterone cannot be made. Treatment replaces both:
Hydrocortisone replaces cortisol (the glucocorticoid)
Fludrocortisone replaces aldosterone (the mineralocorticoid)
⚠️
Board Trap: Phospholipase A2 vs. COX
Cortisol blocks phospholipase A2, which sits UPSTREAM of both prostaglandins AND leukotrienes. NSAIDs block COX, which only blocks prostaglandins. This is why steroids are more powerful anti-inflammatories than NSAIDs: steroids block the whole pathway at the top. NSAIDs only block one branch.
THE MAP
Cortisol at a Glance
Everything in one table. Screenshot this.
HPA Axis: The Cascade and What Breaks It
Follow cortisol from trigger to effect. Each node is a board question.
Trigger: Stress or hypoglycemia detected by the hypothalamus
↓
CRH released from hypothalamus💡CRH = "Come Release Hormone." Hypothalamus sends the starter gun signal to the pituitary.
↓
ACTH released from anterior pituitary corticotrophs
↓
Cortisol released from adrenal cortex zona fasciculata
↓
Metabolic effects
Gluconeogenesis in liver Proteolysis in muscle Lipolysis in fat
Immune effects (IPS)
Inhibit PLA2 (no arachidonic acid) Pacify immune cells Stabilize membranes
↓
Negative feedback: cortisol suppresses both CRH and ACTH💡The factory turns off its own supply chain. Too much cortisol = pituitary and hypothalamus go quiet.
Property
Cortisol
Source
Adrenal cortex, zona fasciculata
Stimulus
ACTH (from anterior pituitary), triggered by CRH (from hypothalamus)
💡The complete cortisol answer: Made in zona fasciculata. Triggered by ACTH from stress/hypoglycemia. Acts via intracellular receptor. Does IPS (immunosuppression) + lipolysis + proteolysis + gluconeogenesis. Permissive for catecholamines. Replaced by hydrocortisone.
CLINICAL TOOL
Decision Tree: Interpreting Cortisol Lab Patterns
Pick the clinical scenario to walk through the workup step by step.
What is the clinical scenario?
Screen first (any one is acceptable): 24-hr urine free cortisol, late-night salivary cortisol (x2), or 1 mg overnight dexamethasone suppression test. If any screen is positive, proceed to localization.
↓
Localization: check plasma ACTH
ACTH-independent: adrenal source (adenoma or carcinoma). Next step: CT adrenal.
ACTH-dependent: pituitary vs. ectopic. Next step: MRI pituitary + high-dose DST (8 mg).
Pituitary source (Cushing disease): the adenoma still responds to very high-dose feedback. Transsphenoidal resection is the treatment.
Ectopic source: the tumor is fully autonomous. Classic culprits: small cell lung cancer (SCLC), carcinoid. Next step: CT chest/abdomen.
Morning cortisol: below 3 = consistent with insufficiency. Between 3 and 18 = borderline, needs stimulation testing.
↓
ACTH stimulation test (cosyntropin): if cortisol stays below 18 at 60 minutes, adrenal insufficiency is confirmed.
↓
Primary adrenal insufficiency (Addison disease): the adrenal gland itself is failing. The pituitary is shouting for help (high ACTH) but the adrenal is not responding.
Secondary adrenal insufficiency: the pituitary is not making enough ACTH (pituitary tumor, exogenous steroid suppression). The adrenal is fine but not getting the signal.
Stress dosing: the HPA axis is suppressed from exogenous steroids and cannot mount its own stress response. Give hydrocortisone 50 to 100 mg IV to cover the procedure or illness. Never abruptly stop chronic steroids without tapering.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.
CHALLENGE
Clinical Questions
5 randomized questions from a pool of 10. Reload for a fresh set.