Five roots, three trunks, three cords, five branches. Tear the top (C5 to C6) and the arm hangs in the waiter's tip. Tear the bottom (C8 to T1) and the hand claws. Learn where the lesion sits and the answer writes itself.
Board Vignette: A 19-year-old wrestler is pinned with his right arm driven down toward his hip while his head is wrenched hard toward the opposite shoulder. In the ER he lets the limb hang at his side, internally rotated with the palm turned backward. The deltoid bulge is flat and he cannot lift the arm away from his body, bend the elbow, or turn the palm up. Sensation is dulled over the outer shoulder and the lateral forearm down to the thumb, and the biceps reflex is gone. Grip strength and the small muscles that spread the fingers are completely normal. Which action is MOST impaired in this patient?
A. Abduction of the humerus
B. Pronation of the forearm
C. Flexion of the fingers
D. Abduction and adduction of the fingers
Downward traction on the arm with the head forced away has avulsed the upper trunk (C5 to C6), the classic Erb-Duchenne palsy. The deltoid (axillary nerve) and supraspinatus (suprascapular nerve) both draw their fibers from C5 to C6, so abduction of the humerus is the first action to die, alongside elbow flexion and external rotation. Pronation is the trap: the arm rests pronated, but the action of pronation runs on pronator teres (median nerve, C6 to C7), which survives a pure upper-trunk tear. That is the same reason grip and finger spread (C8 to T1, the lower-trunk territory of Klumpke) stay normal here. Upper trunk kills abduction and external rotation, not the hand.
The Plexus Map
Tap any node to see what it carries and what breaks when it is cut. Then switch to Lesion mode and watch the upper trunk (Erb) and the lower trunk (Klumpke) light up the two halves of the arm.
First, what is a root here?
Every spinal nerve leaves the spine and splits into two branches. The small dorsal ramus turns backward to supply the deep muscles of the back and a thin strip of skin over the spine. The large ventral ramus carries the rest: motor and sensory fibers for the front and sides of the body and the whole limb.
The roots of the brachial plexus ARE the ventral rami of C5 through T1. Dorsal rami never join a plexus, only ventral rami do. That weaving of ventral rami is exactly why one trunk lesion drops several muscles from different spinal levels at once.
Tap any node
StartGreen is the upper level (C5 to C6), blue is the middle (C7), red is the lower level (C8 to T1), purple are the cords, gold are the terminal branches. Tap one to see what it carries.
Upper C5 to C6 (Erb)
Middle C7
Lower C8 to T1 (Klumpke)
The real plan of the brachial plexus: five roots (C5 to T1) gather into three trunks, split into divisions, regroup into three cords, then fan into the terminal branches. Tap to expand.
From the Attending
Everything in this topic is geography. The top of the plexus (C5 and C6) feeds the shoulder and the outer arm. The bottom (C8 and T1) feeds the hand. So an injury that yanks the head away from the shoulder tears the top, and the deltoid, biceps, and external rotators die: the waiter's tip. An injury that yanks the arm overhead tears the bottom, and the small hand muscles die: the claw. Tell me where the lesion is and I will tell you what the arm does. Find the level first, every time.
Erb vs Klumpke vs the Cords
Two named palsies at the ends of the plexus, and the cords in between. Tap a tab.
ERB
KLUMPKE
CORDS
BRANCHES
Erb-Duchenne Palsy
Upper trunk, C5 to C6, the waiter's tip
LesionUpper trunk (C5 to C6)
InjuryShoulder forced DOWN and head AWAY: a fall onto the shoulder, or shoulder dystocia at birth
Dead musclesDeltoid and supraspinatus (abduction), biceps and brachialis (flexion), infraspinatus (external rotation)
PostureArm adducted, internally rotated, forearm extended and pronated: the waiter's tip
ReflexesBiceps and brachioradialis reflexes lost
Board trapPronation is spared: pronator teres is median, C6 to C7
Klumpke Palsy
Lower trunk, C8 to T1, the claw hand
LesionLower trunk (C8 to T1)
InjuryArm yanked OVERHEAD: grabbing a branch in a fall, or upward traction on the arm at birth
Dead musclesIntrinsic hand muscles (interossei, lumbricals, thenar, hypothenar) plus long finger flexors
PostureTotal claw hand: MCPs extended, fingers flexed, thumb cannot oppose
Look forHorner syndrome (ptosis, miosis, anhidrosis) if T1 sympathetics are torn
Board trapShoulder and elbow are fine: the hand is the whole story
The Three Cords
Named for how they sit around the axillary artery
Lateral cordMusculocutaneous plus the lateral root of the median nerve
Posterior cordAxillary and radial nerves (all the extensors)
Medial cordUlnar plus the medial root of the median nerve
Median nerveBuilt from BOTH the lateral and medial cords: a lateral root and a medial root
Board trapPosterior cord = extensors. A torn posterior cord drops wrist and elbow extension
The Five Terminal Branches
Where the cords end and the named nerves begin
MusculocutaneousElbow flexion (biceps, brachialis) and lateral forearm sensation
AxillaryShoulder abduction (deltoid) and the regimental badge patch of sensation
RadialWrist and finger extension: a lesion gives wrist drop
MedianForearm pronation, wrist flexion, thumb opposition, lateral three and a half digits
UlnarMost intrinsic hand muscles, finger spread, and the medial one and a half digits
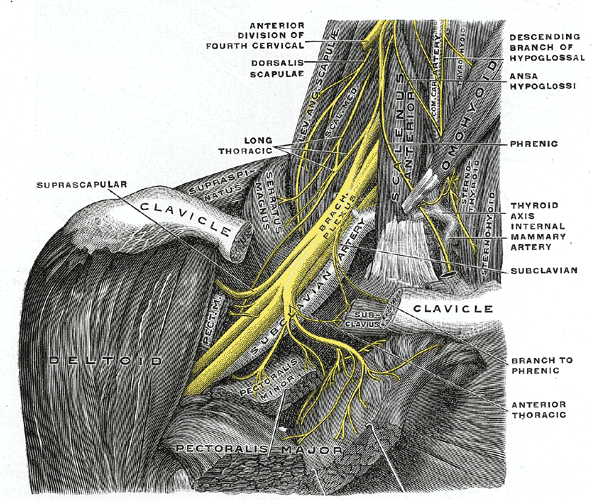
The brachial plexus in the neck and axilla: the trunks emerge between the scalene muscles, with the suprascapular nerve peeling off the upper trunk early. Tap to expand.
From the Attending
Two ends, two pictures. Erb is the shoulder, Klumpke is the hand. The upper trunk runs abduction, flexion, and external rotation, so when it tears, the arm rolls into the waiter's tip. The lower trunk runs the small muscles of the hand, so when it tears, the hand claws and you go looking for a droopy eyelid from the T1 sympathetics. Top of the plexus, top of the arm. Bottom of the plexus, the hand. Anchor the two ends and the cords fall into place.
Roots to Branches
The five layers in order, and the one fact that pins each. Read the layer, predict what it does, then tap that row to check it.
read the layer, call the key fact, then tap that one row to reveal it
Layer
What it is
Key fact for the exam
Roots (C5 to T1)
Five ventral rami, between the scalene muscles
Long thoracic nerve (C5 to C7) leaves here: injury gives a winged scapula
Trunks (3)
Upper (C5 to C6), Middle (C7), Lower (C8 to T1)
Upper trunk tear is Erb, lower trunk tear is Klumpke
Divisions (6)
Each trunk splits into an anterior and a posterior division
Lateral, Posterior, Medial, named off the axillary artery
Posterior cord becomes the axillary and radial nerves: the extensors
Branches (5)
Musculocutaneous, Axillary, Radial, Median, Ulnar
Median is built from two cords; ulnar is the lower-trunk, claw-hand nerve
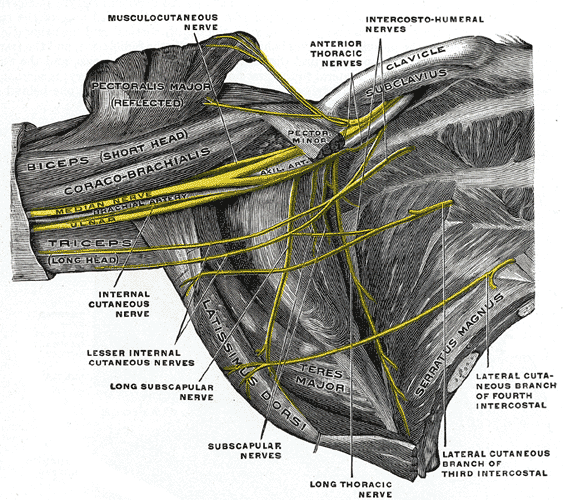
The cords become the named nerves of the arm: the musculocutaneous diving into the biceps, the median and ulnar running to the hand, the radial wrapping behind the humerus. Tap to expand.
From the Attending
Walk it top to bottom: Roots, Trunks, Divisions, Cords, Branches. Most board questions live at the trunk row, because that is where the two named palsies sit. But notice the root row: the long thoracic nerve and the dorsal scapular nerve come straight off the roots, before the trunks even form, which is why a winged scapula is a root-level problem and not a cord problem. The level of the lesion is the diagnosis. Learn the order and you can place any deficit on the map.
Localize the Lesion
Commit to a level before the answer drops.
1
A patient has a weak, numb arm after a traction injury. First fork: which part of the limb is dead?
Shoulder and outer arm: cannot abduct or flex the elbow
The hand: small hand muscles weak, fingers clawing
The scapula wings off the back when pushing a wall
2
Shoulder and outer arm. So this is the top of the plexus. What is the posture and reflex pattern?
Arm adducted and internally rotated, forearm pronated, biceps reflex gone: the waiter's tip
Only the deltoid is weak, with a numb patch over the shoulder tip, elbow flexion intact
3
The hand. So this is the bottom of the plexus. What else is on the exam?
Total claw hand after the arm was yanked overhead, with a droopy eyelid and small pupil
Clawing of only the ring and little fingers after a blow to the medial elbow
From the Attending
Notice the funnel. The first fork is where in the arm. The second fork is how complete the lesion is. A whole upper trunk gives the waiter's tip; an isolated axillary nerve gives only a weak deltoid and a numb shoulder patch. A whole lower trunk gives a total claw with a Horner; an isolated ulnar nerve at the elbow gives only a partial claw of the last two fingers. Trunk versus single nerve is the difference between a wide deficit and a narrow one. Read how much is gone.
Wrong Answer Autopsy
Every distractor has a reason it tempts you. Tap to flip and find it.
Pronation of the Forearm
Why it feels right: the arm hangs pronated in the waiter's tip, so pronation looks like the dead movement.
The Trap: you see a pronated arm and conclude pronation is what failed.
flip for the rule →
The Rule
The problem
Pronator teres runs on the median nerve from C6 to C7. A pure upper-trunk lesion (C5 to C6) largely spares it, so pronation actually still works. The forearm LOOKS pronated because the supinators (biceps, supinator) are dead and leave it resting that way.
Keep it straight
The arm rests pronated because supination is lost, not because pronation is. Upper trunk kills abduction and elbow flexion, not pronation.
Lower Trunk (Klumpke)
Why it feels right: it is the other named plexus palsy, so it shows up on every brachial plexus question.
The Trap: a shoulder injury, and you reach for the famous hand palsy.
flip for the rule →
The Rule
The problem
Klumpke is C8 to T1: the small hand muscles, the claw, and a possible Horner. It comes from upward traction on an abducted arm, not a blow to the shoulder. A lateral arm and thumb that are numb with a dead deltoid are upper-trunk territory.
Keep it straight
Klumpke is the hand and the eyelid. If the hand is fine and the shoulder is dead, you are at the upper trunk, not the lower.
Axillary Nerve Alone
Why it feels right: the deltoid is weak and the deltoid is the axillary muscle, so a single nerve seems to fit.
The Trap: you call a wide C5 to C6 deficit an isolated axillary nerve palsy.
flip for the rule →
The Rule
The problem
An isolated axillary nerve lesion kills only the deltoid and numbs a small patch over the shoulder. It does NOT touch the biceps reflex or the lateral forearm. When elbow flexion and the biceps reflex are also gone, the lesion is upstream at the whole upper trunk.
Keep it straight
Axillary alone is just the deltoid and a shoulder patch. Add a dead biceps and lost reflex and you are at the upper trunk.
Long Thoracic Nerve
Why it feels right: it is a C5 to C7 nerve, so it overlaps the upper levels and sounds plausible.
The Trap: an upper plexus stem, and you pick the winged-scapula nerve.
flip for the rule →
The Rule
The problem
The long thoracic nerve supplies the serratus anterior. Its injury gives a winged scapula and trouble raising the arm above the head, not a dead deltoid, biceps, and a numb thumb. It also branches off the roots, before the trunks form.
Keep it straight
Long thoracic equals winged scapula. No winging, no serratus story, then this is not your nerve: look at the upper trunk.
The musculocutaneous nerve to the elbow flexors and the median and ulnar nerves running to the hand. The median carries pronation from C6 to C7, which is why a pure upper-trunk lesion leaves pronation working. Tap to expand.
Memory Hooks
Predict first, then tap to unblur.
🧾
Read the layers in order
Roots, Trunks, Divisions, Cords, Branches.Randy Travis Drinks Cold Beer.Five layers, lateral to the cord. Place any deficit by asking which layer it sits in.
tap to reveal
🥇
Top of plexus, top of arm
Erb is C5 to C6: the shoulder.Upper trunk runs abduction (deltoid, supraspinatus), elbow flexion (biceps), and external rotation. Tear it and the arm rolls into the waiter's tip. Mechanism: shoulder pushed down, head pulled away.
tap to reveal
🦦
Bottom of plexus, the hand
Klumpke is C8 to T1: the hand.Lower trunk runs the small hand muscles. Tear it and the hand claws. Mechanism: arm yanked overhead. Hunt for a Horner (ptosis, miosis, anhidrosis) from the T1 sympathetics.
tap to reveal
🤳
The pronation trap
The waiter's tip arm rests pronated, but pronation is not what failed.Pronator teres is median, C6 to C7, spared in a pure upper-trunk lesion. The forearm sits pronated because the supinators (biceps, supinator) are dead. Lost action is supination, not pronation.
tap to reveal
🥘
Posterior cord is the extensors
Posterior cord = axillary + radial.Everything that extends or abducts the limb behind. A torn posterior cord drops the deltoid and the wrist together. Anterior divisions feed flexors, posterior divisions feed extensors.
tap to reveal
👀
A droopy eyelid means T1
Horner with a clawed hand = lower trunk.The sympathetic chain to the eye climbs through T1. A lower-trunk avulsion that takes T1 can take the sympathetics with it, giving ptosis, miosis, and anhidrosis on the same side. A shoulder Erb injury never does this.
tap to reveal
The upper plexus in the posterior triangle of the neck. The suprascapular nerve to the supraspinatus comes straight off the upper trunk, which is why shoulder abduction fails so early in Erb palsy. Tap to expand.
Prove It
Original board-style vignettes. One at a time. Tap each teaching beat to reveal the chain.
From the Attending
These stems hide the level behind a familiar word. Find the level first. Lateral arm, dead deltoid and biceps, lost biceps reflex is the upper trunk: Erb. Clawed hand, dead intrinsics, a droopy eyelid is the lower trunk: Klumpke. Then check what the question is actually asking, because the pronated waiter's-tip arm is built to make you pick pronation. The posture is a clue to the dead supinators, not the dead pronators. Right click or long press to cross out a choice, double tap to highlight one. Don't overthink it.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.