Bones approximate, bones separate, or bones stay locked. Concentric, eccentric, isometric, and isolytic. That distinction drives OMM and MET. Every time.
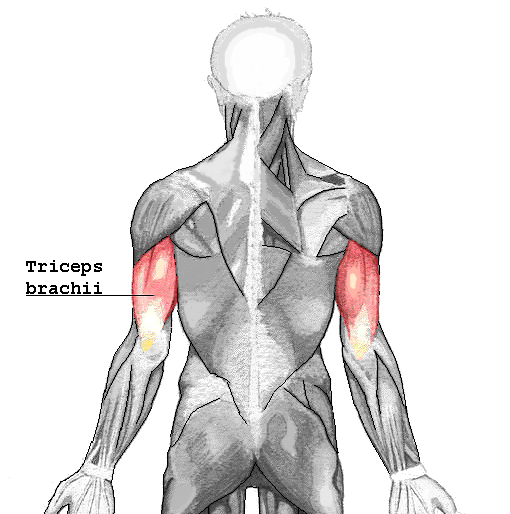
A collegiate weightlifter reports sharp pain at the posterior elbow during the lockout phase of an overhead press. On physical exam, he experiences discomfort while actively contracting the triceps muscle to extend the forearm against resistance. What type of muscle contraction occurs as the triceps fibers actively shorten under this load?
A. Concentric contraction
B. Eccentric contraction
C. Isokinetic contraction
D. Isolytic contraction
E. Isometric contraction
Acknowledge the trap: Yes, the joint is extending (straightening), which makes you think of pushing or stretching. But look at the muscle itself. The triceps is contracting to lift the load, which means its fibers are actively shortening.
Concentric contraction occurs when a muscle shortens under constant tone, regardless of the joint's direction of movement.
From the Attending
"Always look at the muscle belly, not the joint movement. Triceps shortens during elbow extension. Biceps shortens during elbow flexion. If the active muscle shortens to move the load, it is a concentric contraction. Every time."
The Cross-Bridge Cycle, Step by Step
Tap a step. Watch the actin−myosin cycle morph. Every contraction type below rides this loop.
Step 1 of 5
At Rest · Tropomyosin Blocks
Calcium is locked in the sarcoplasmic reticulum. Tropomyosin sits across the actin binding sites. The myosin head is cocked, ATP-loaded, waiting.
Rule: ATP is needed TWICE · once to detach (rigor releases) and once to recock the head. No ATP = rigor mortis.
The Five Contraction Types
Tap a card to expand. Each type has a unique animation showing how the muscle behaves.
Concentric
Muscle shortens · Attachments approximate
Tap to expand
Concentric Isotonic
What Happens
Patient's active force overpowers the load. Muscle fibers shorten, pulling origin and insertion closer together.
Length / Tone
Length decreases · Tone stays constant (isotonic)
MET Use
Concentric MET strengthens weak, inhibited antagonist muscles. Patient's force exceeds physician counterforce.
Watch For
Do not confuse with joint extension. Concentric means the active muscle shortens, regardless of joint direction.
Eccentric
Muscle lengthens under tension · Load wins
Tap to expand
Eccentric Isotonic
What Happens
External load overpowers the active muscle. Origin and insertion move farther apart while the muscle fires to decelerate.
Length / Tone
Length increases (lengthens) · Tone stays constant (isotonic)
Stem Signals
"Lowering a weight slowly," "walking downstairs," "deceleration after throwing." The muscle is actively working, not resting.
Clinical Pearl
Eccentric contractions cause the most DOMS (delayed onset muscle soreness) and the highest CK elevations. High-yield correlation.
Isometric
Same length · Tension rises · No movement
Tap to expand
Isometric
What Happens
Patient force equals physician counterforce. Distance between origin and insertion remains constant. Tension rises without movement.
Length / Tone
Length constant · Tone increases
MET Use
Post-isometric relaxation (PIR): the workhorse MET. Also used for reciprocal inhibition when the agonist is too painful to contract directly.
Reflex
GTO fires → Ib afferent → inhibitory interneuron → alpha motor neuron suppression → autogenic inhibition. That is the PIR mechanism.
Isolytic
Physician overpowers · Forced stretch
Tap to expand
Isolytic
What Happens
Physician's force overpowers the patient's voluntary contraction. The muscle is forced to lengthen while actively firing. Micro-tears break fibrotic tissue.
Length / Tone
Length forced to increase · Tone constant/high
Indication
Chronic fascial restrictions and fibrotic contractures that do not respond to PIR. Never for acute spasm.
vs Eccentric
Both lengthen the muscle, but in eccentric the load wins naturally. In isolytic, the physician deliberately overpowers. That is the board differentiator.
Isokinetic
Constant speed · Machine-controlled velocity
Tap to expand
Isokinetic
What Happens
Dynamometer matches resistance to patient's force at every angle, maintaining a locked angular velocity throughout the entire arc.
Speed / Length
Joint speed constant throughout · Length changes (shortens or lengthens depending on phase)
Clinical Use
Rehabilitation dynamometry and sports medicine strength testing. Requires specialized equipment.
Stem Signals
"Constant speed," "locked velocity," "dynamometer." Does NOT occur naturally. Almost never the MET answer, but a common distractor.
The Trap: Isolytic vs Standard Eccentric
clinical medicine love to test the differentiator. Both involve a muscle lengthening under tension. However, in a standard eccentric contraction, the muscle itself controls the lengthening against a load (like lowering a dumbbell). In an isolytic contraction, the lengthening is forced by an external force (the physician) that actively overpowers the patient's voluntary muscle contraction. Isolytic = physician wins and overpowers the patient's muscle.
Triceps Brachii · tap to view
Sarcomere Shortened · tap to view
Sarcomere Lengthened · tap to view
Cross-Bridge Cycle · tap to view
Triceps (Lateral) · tap to view
Sarcomere & Arm Simulator
Tap a contraction state to visualize the macroscopic movement and microscopic filament alignment.
From the Attending
"Concentric isotonic contraction. The patient's active force overpowers the resistance, so muscle fibers shorten and attachments approximate. In concentric MET, the patient's force exceeds the physician's counterforce. Decreased muscle length. Every time."
Build a MET Protocol
Walk through a real clinical scenario step by step. Choose the correct action at each decision point.
Step 1 of 5: Identify
A 32-year-old office worker presents with right-sided neck pain and restricted left rotation. Structural exam reveals C4 rotated right, sidebent right (C4 FRSr). Which of the following best describes the position of ease?
Rotated right, sidebent right (the direction it moves freely)
Rotated left, sidebent left (the direction of restriction)
Neutral position with no rotation
The somatic dysfunction is named for the position of ease. C4 FRSr means it rotates right and sidebends right easily. Its restriction is in the opposite direction: rotation left, sidebending left.
Step 2 of 5: Position
You decide to use PIR MET (direct technique). To engage the restrictive barrier before the patient contracts, which direction must you move C4?
Rotate right, sidebend right (into ease)
Rotate left, sidebend left (into the barrier)
Flex the neck fully, then rotate
Direct technique means engaging the restrictive barrier. Since the restriction is rotation left and sidebending left, you must position C4 into that direction. Direct = into the bind.
Step 3 of 5: Contract
C4 is now at the restrictive barrier. You instruct the patient to contract. Which direction should the patient push?
Toward the ease (rotate right, sidebend right) against your matched counterforce
Into the barrier (rotate left) to stretch the muscle further
In any direction, as long as force is applied
The patient contracts toward ease (away from the barrier). You match their force exactly: isometric contraction. No movement occurs. The restricted agonist muscle fires, loading the Golgi tendon organs.
Step 4 of 5: Relax
The patient holds for 3 to 5 seconds. What is the correct sequence after the contraction ends?
Immediately push to the new barrier without waiting
Instruct the patient to relax completely, exhale, then gently take C4 to the new barrier
Have the patient contract again in the same position
After contraction, the post-isometric relaxation window opens. The patient must fully relax (exhale augments this via respiratory assist). Then, gently move C4 to the new, improved restrictive barrier. Pushing before relaxation triggers protective spasm.
Step 5 of 5: Repeat
How many cycles should you perform, and what physiological mechanism made the muscle relax?
3 to 5 repetitions, each engaging a progressively deeper barrier. The mechanism: isometric contraction loads the Golgi tendon organ, which fires Ib afferents to inhibitory interneurons, suppressing alpha motor neuron output to the same muscle. Autogenic inhibition. That is PIR.
Protocol Complete
You built a full PIR MET from dysfunction identification through repetition. The five steps: Identify → Position at barrier → Patient contracts toward ease (isometric) → Relax and engage new barrier → Repeat 3 to 5 times.
From the Attending
"The board move is matching the contraction to the goal. Hypertonic muscle, want relaxation → isometric MET (post-isometric relaxation via GTO autogenic inhibition, or reciprocal inhibition by contracting the antagonist). Chronic fibrotic restriction → isolytic (physician overpowers patient force, stretches the fascia). Weak inhibited muscle → concentric MET to strengthen. Pick the lever that matches the lock. Every time."
PIR vs RI Decision Tree
Follow the clinical logic to determine which MET approach fits the patient.
1
Is the target hypertonic muscle acutely painful or injured (too painful to contract directly)?
2
Use Reciprocal Inhibition. Contract the antagonist isometrically. The reflex pathway relaxes the target agonist without requiring it to fire.
2
Is the restriction chronic and fibrotic (failed multiple PIR sessions)?
3
Is the primary goal to relax a hypertonic agonist, or to strengthen a weak, inhibited antagonist?
Clinical Scenario Cards
Tap each card to reveal the contraction type and clinical reasoning. Tap again to flip back.
Post-Op Knee Rehab
8 weeks post-ACL reconstruction. PT introduces a Biodex dynamometer at 60 degrees per second. What contraction type?
Isokinetic
The dynamometer maintains constant angular velocity throughout the arc. Isokinetic contractions require specialized machine control and do not occur naturally.
Stem says "constant speed" or "dynamometer" = isokinetic.
Tap to flip back
Cervical Somatic Dysfunction
C5 rotated left, restricted rotation right. Physician matches patient's force exactly. No movement. Which contraction?
Isometric (PIR)
Patient contracts toward ease against perfectly matched counterforce. Distance between origin and insertion remains constant. Tension rises without movement. GTO fires autogenic inhibition.
Stem says "matched force," "no movement" = isometric.
Tap to flip back
Achilles Tendinopathy Rehab
Patient slowly lowers heel off step edge, controlling descent against gravity. The gastrocnemius lengthens while actively firing. Which contraction?
Eccentric
The muscle actively fires but the gravitational load exceeds its force, causing controlled lengthening. Eccentric rehab is the gold standard for Achilles tendinopathy.
5-year hamstring contracture. PIR failed three times. Physician overpowers the patient's active flexion contraction, forcing the muscle to lengthen. Which contraction?
Isolytic
The physician's force exceeds the patient's voluntary contraction, forcing the muscle to stretch while actively firing. This breaks chronic, dense fascial restrictions. Never for acute spasm.
Post-stroke patient with weak quadriceps (2/5 strength). The patient actively shortens the quad against light physician resistance. Which contraction?
Concentric
The patient's force exceeds the physician's light resistance, allowing active muscle shortening. Concentric MET retrains and strengthens inhibited antagonist muscles.
Stem says "strengthen," "weak," "patient's force exceeds" = concentric MET.
Tap to flip back
Memory Hooks: Force Lab
Tap the board phrase. Watch who wins the tug of war, whether the joint moves, and why that answer survives.
Force balance
PT
DO
Patient force = physician force. No joint motion.
Iso-metric = same length
What moved?
Nothing. The joint does not move because both forces match.
Exam tell
The stem says matched counterforce, no movement, or post-isometric relaxation.
This is the workhorse MET.
Respiratory Assist vs. Oculocephalogyric Reflex
Two augmentation tools clinical medicine love to confuse. Respiratory assist: the patient exhales during the relaxation phase to augment vertebral/rib mobility. Oculocephalogyric (eye-head) reflex: the patient looks in the direction of the desired motion to facilitate cervical or cranial segment movement. Both are add-ons to a standard isometric MET, not replacements for it.
Board Walkthrough
27 original clinical vignettes. One at a time. Highlight selection or cross-out answers exactly like on the real clinical medicine.
From the Attending
"OMM stems are pattern recognition. Read the last sentence first. Which contraction type? → ask: did the muscle shorten (concentric), lengthen with control (eccentric), stay the same length (isometric), get forced to stretch (isolytic), or run on a machine (isokinetic)? Which MET? → match the goal: relax = isometric/PIR, fibrosis = isolytic, weak = concentric. Cross out the distractor that does not match the patient's direction of force. Do not memorize 27 vignettes. Learn the 5 lever rules."
Tip: Double-tap / double-click to highlight. Right-click / long-press to cross-out options.
Progress saves in a cookie on this device. Shuffle & Restart clears it.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.