The Mechanism
What HVLA actually is, how the pop happens, and how it differs from other OMM techniques
HVLA is a direct technique. You take up all the slack in the restricted direction until you reach the restrictive barrier, then apply a short, high-velocity thrust through that barrier with a low amplitude of movement. The key: you go into the restriction, not away from it.
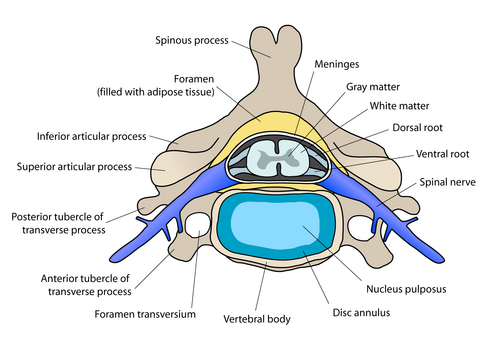
The audible and palpable "pop" is nitrogen cavitationRapid drop in intra-articular pressure creates a gas bubble in the synovial fluid that collapses, producing the audible pop. Same physics as cracking your knuckles.. The joint spaces briefly gape, stretch the periarticular capsule and ligaments, and stimulate mechanoreceptors that reflexively inhibit paraspinal muscle hypertonicity. The pop is satisfying but NOT required for therapeutic benefit.
Watch where the thrust actually travels. Neutral sits in the middle of the easy range. In a healthy joint, motion stops at the physiologic barrier (the active end range). The hard stop past it is the anatomic barrier (bone on bone: cross it and you tear tissue). In dysfunction, a restrictive barrier forms early, short of the physiologic limit. HVLA takes up slack to the restrictive barrier, then thrusts a few millimeters through it toward the physiologic barrier. That gap is where cavitation happens.
Absolute Contraindications
The highest-yield section for clinical practice. Know all nine. Cold.
Relative Contraindications
Pause, modify, or defer. Not never. But not without careful thought.
Relative contraindications mean HVLA is possible with modification or after a risk-benefit analysis. The dysfunction may still be treated with gentler techniques (MET, counterstrain, myofascial) while HVLA is deferred.
The Five Parameters
Every HVLA attempt requires five things to be set before the thrust is delivered
HVLA is not "just crack the back." Five technical parameters must be precisely established before the thrust. Getting any one wrong means either therapeutic failure or patient harm.
Tap a technique to compare how each one approaches the same restricted segment.
HVLA: thrust through the barrier
- Direction: direct, into the restriction toward the physiologic barrier
- Force source: the physician, a single high-velocity, low-amplitude thrust
- Endpoint: mechanical gapping and cavitation; correction of the dysfunction
- Most contraindications of any technique: fragile bone, instability, bleeding risk
Muscle Energy: patient does the work
- Direction: direct, engaging the barrier, then advancing with each repetition
- Force source: the patient, isometric contraction for 3 to 5 seconds
- Endpoint: post-isometric relaxation lets the physician take up new slack, repeat about three times
- Low force: a safe alternative when HVLA is contraindicated
Counterstrain: move away from the pain
- Direction: indirect, away from the restrictive barrier into a position of ease
- Force source: passive positioning held about 90 seconds over a tender point
- Endpoint: resets aberrant proprioceptive firing; no thrust
- Gentle: appropriate in fragile patients
Myofascial Release: follow the tissue
- Direction: direct or indirect, loading or unloading the fascial restriction
- Force source: sustained physician pressure following tissue creep
- Endpoint: fascial release without a high-velocity load
- Low force: another safe substitute when a thrust is contraindicated
Can I HVLA?
Read the vignette. Reveal the clues. Make the call.
Thrust or do not. Tap a finding below, then drop it into the right bin. Absolute means HVLA is never done at that site, full stop. Relative means pause, modify, or defer to a gentler technique.
One more case, branch by branch. Answer each node to unlock the next.
Quiz
Eight original clinical questions · Tap to answer
Which statement best characterizes the appropriateness of HVLA for this patient?
Osteopenia (T-score -1.0 to -2.5) is NOT the same as osteoporosis (T-score below -2.5). The absolute contraindication is SEVERE osteoporosis, which carries significant pathological fracture risk from even minor forces. This patient has osteopenia managed with bisphosphonates and no fractures. Thoracic HVLA at T6 is appropriate.
Break it down: A is wrong because osteopenia alone is not an absolute CI. C overstates the relative risk without sufficient clinical basis. D is incorrect because bisphosphonate therapy actually reduces fracture risk by treating bone loss; it is not itself a contraindication to manipulation.
A positive test is best interpreted as:
The vertebral artery screening test detects compromise of the vertebral arteries with positional challenge. A positive result (nystagmus, vertigo, diplopia, or syncope during positioning) suggests that cervical HVLA in that direction could compress the vertebral artery and cause posterior circulation stroke. This is a RELATIVE contraindication: defer cervical HVLA, but gentle non-thrust techniques (MET, soft tissue) may still be used.
Break it down: An absolute contraindication would prohibit all cervical manipulation, which is not the case here. The positive test does not mandate emergent neurology unless symptoms are severe or persistent after repositioning. In practice, a positive test means no high-velocity cervical manipulation.
What is the most appropriate next step?
Acute disc herniation with active radiculopathy is a relative contraindication to HVLA because a thrust could worsen nerve root compression. Cauda equina syndrome (bilateral weakness, bowel/bladder) would make this absolute. This patient has unilateral S1 radiculopathy, which is relative. Use gentler techniques (MET, myofascial, counterstrain) while the disc is acute. Once the acute phase resolves, reassessment for HVLA is appropriate.
Break it down: Reducing amplitude does not eliminate the risk because the high velocity is still present and can worsen the disc protrusion. Informed consent is a process, not a clinical override of a contraindication.
What is the most appropriate next action?
If the first HVLA attempt does not produce cavitation or correction, re-examine to confirm the dysfunction persists, re-engage the barrier carefully, and attempt one more thrust. If the second attempt also fails, switch to an alternative technique (MET, counterstrain). The rule is: two attempts maximum, then switch.
Break it down: Multiple consecutive thrusts increase injury risk and allow insufficient recovery time. Increasing velocity means more force, not better specificity, and is not the correct response to a failed attempt. The absence of an audible pop does not mean the technique failed: therapeutic benefit can occur without cavitation, and the endpoint is functional correction, not sound production.
Which of the following correctly describes the direction of the HVLA thrust and the classification of this technique?
HVLA is a direct technique: the physician takes up all slack in the restricted direction across all three planes (flexion/extension, rotation, sidebending), engages the restrictive barrier, then delivers a high-velocity, low-amplitude thrust through that barrier. Going into the restriction is what distinguishes direct techniques from indirect ones. Counterstrain and myofascial release move away from the barrier (indirect). MET uses the patient's voluntary isometric force to move the barrier -- HVLA does not require patient effort. Delivering the thrust before engaging the barrier is a technique error that produces no therapeutic benefit and may harm the patient.
Break it down: HVLA is direct -- take up slack, engage barrier, thrust through it. Always through, never away.
Which statement best describes the appropriate management of her cervical somatic dysfunction?
Hypermobility (joint instability) is a relative contraindication to HVLA. The mechanism: HVLA works by gapping and stretching the periarticular capsule and ligaments, firing mechanoreceptors in the joint capsule. In an already-hypermobile joint, the capsule and ligaments are already excessively lax. More stretching worsens instability, not treats it. The correct approach is to use stabilizing techniques: MET (which uses isometric contraction to strengthen the stabilizing muscles), soft-tissue work, or myofascial release. HVLA is a relative, not absolute, contraindication for hypermobility -- absolute CIs are structural (fracture, RA atlantoaxial, cord compression, anticoagulation). Deferring all OMM is incorrect; the patient still has somatic dysfunction that can be addressed with appropriate non-HVLA techniques.
Break it down: hypermobility = relative CI for HVLA. Use MET and stabilizing techniques instead.
What is the most appropriate course of action regarding HVLA?
Metastatic bone disease to the spine is an absolute contraindication to HVLA at that site -- regardless of neurological status, gentleness, or informed consent. A lytic lesion at T7 in a prostate cancer patient has severely compromised the structural integrity of the vertebral body. HVLA can cause an immediate pathological fracture with cord compression, even with minimal force. The absence of neurological deficits does not make it safe -- it simply means the catastrophe has not happened yet. Night pain plus weight loss plus prior cancer history is the red-flag triad for spinal metastases that every physician must screen before ANY OMM. Informed consent does not override an absolute contraindication. MET is appropriate for the somatic dysfunction while oncology is consulted urgently.
Break it down: bone mets plus HVLA equals pathological fracture. Night pain plus cancer history equals red flag. Absolute contraindication.
Which of the following best describes the role of HVLA in her management?
Active inflammatory flare (ankylosing spondylitis, psoriatic arthritis, gout) is a relative contraindication to HVLA. During active inflammation, periarticular structures are acutely inflamed, vascularized, and fragile. HVLA during a flare can worsen inflammation, cause microtears, and in advanced ankylosing spondylitis (bamboo spine), cause fracture through a rigidly fused segment. The correct approach is to wait until the flare is medically controlled, then reassess. If her disease is in remission and imaging shows no bamboo spine or fractures, HVLA could be considered with appropriate modification. Ankylosing spondylitis is not an absolute CI under all circumstances -- the active flare and the structural changes (if present) drive the contraindication level. HVLA does not reduce inflammation; it is a mechanical technique without direct anti-inflammatory effect.
Break it down: active inflammatory flare equals relative CI for HVLA. Control the inflammation first, then reassess.
Board Walkthrough
Six original clinical vignettes, shuffled and never-repeating. Right-click or long-press to cross out. Double-click or double-tap to highlight. Answer, then tap the wrong choices to learn why.
