A 31-year-old with MS, a stiff left leg, and five nerves that could be the culprit. Only one actually drives hip flexion.
CLINICAL CHALLENGE
A 31-year-old woman with relapsing-remitting MS presents with left leg cramps worsening over 3 months. Exam shows increased tone in the left thigh with involuntary hip flexion. Reflexes are brisk at the left knee. She asks about a nerve block to reduce the spastic pulling. Which nerve innervates the muscles causing her spastic hip flexion?
A. Inferior gluteal nerve
B. Superior gluteal nerve
C. Femoral nerve
D. Obturator nerve
E. Sciatic nerve
The femoral nerve (L2-L4) innervates the iliopsoas (primary hip flexor) and the quadriceps (knee extensor). In MS, upper motor neuron lesions cause increased tone in muscles these nerves supply. Since the spasticity is pulling the hip into flexion ↑, the femoral nerve is the one driving the problem. Blocking any other nerve would remove a counterforce and potentially make the spastic flexion worse.
The Five Lower Extremity Nerves
Tap each nerve to see what it controls. Every one comes from the lumbosacral plexus, but they split into very different jobs.
Femoral Nerve 🔑NAVEL: In the femoral triangle, from lateral to medial: Nerve, Artery, Vein, Empty space (canal), Lymphatics. The nerve is most lateral. Needle for nerve block goes lateral to the arterial pulse.
L2 · L3 · L4
Motor: Hip flexion (iliopsoas) + knee extension (quads). ↑ Think: kicking a soccer ball uses both motions.
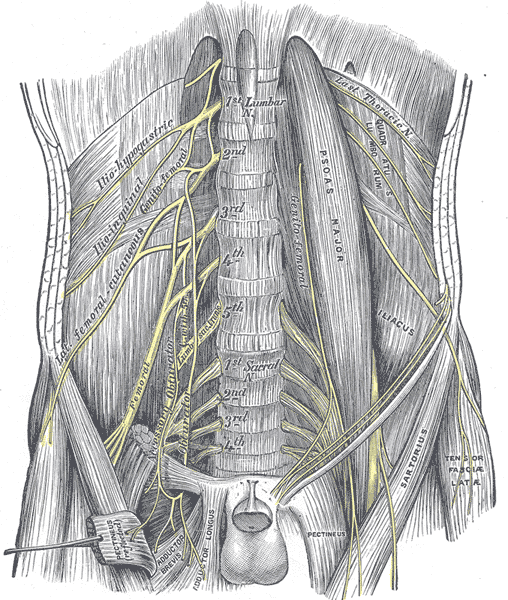
Path: Exits lateral border of psoas major, passes under the inguinal ligament into the femoral triangle. MIXED
Obturator Nerve
L2 · L3 · L4
Motor: Hip adduction (adductor longus, brevis, magnus). Think: squeezing your knees together on a horse.
Sensory: Small patch on the medial thigh.
Path: Exits medial border of psoas, travels through the obturator foramen into the medial thigh compartment. MIXED
Sciatic Nerve 🔑Steppage gait = Sciatic/Peroneal. Sciatic injury causes foot drop (common peroneal branch). Patient lifts knee high to clear the floppy foot. Waddling gait = superior gluteal. Steppage gait = sciatic/peroneal. Different gaits, different nerves.
L4 · L5 · S1 · S2 · S3
Motor: Hamstrings (knee flexion, hip extension) + everything below the knee via tibial and common peroneal branches.
Sensory: Posterior thigh (via posterior cutaneous nerve), lateral leg, sole of foot.
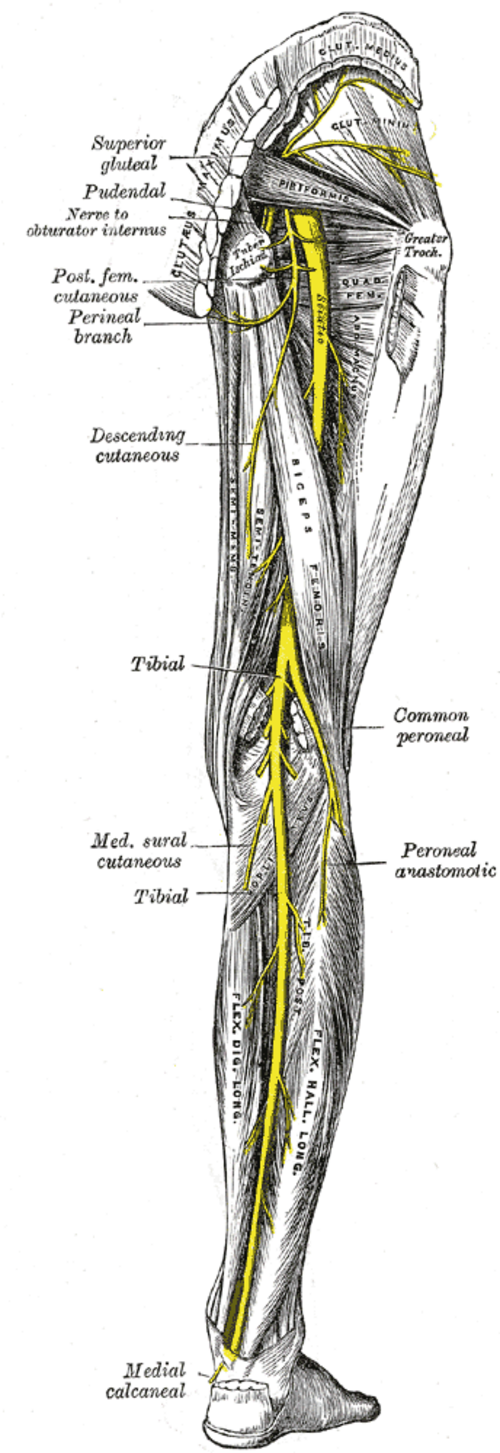
Path: Largest nerve in the body. Exits greater sciatic foramen below piriformis, descends posterior thigh. Splits into tibial + common peroneal at the popliteal fossa. MIXED
Superior Gluteal Nerve 🔑Above vs Below piriformis: Superior gluteal exits ABOVE piriformis, goes to abductors. Inferior gluteal exits BELOW, goes to glut max. Same foramen, different floors. Board question: "exits above piriformis" = superior gluteal.
L4 · L5 · S1
Motor: Hip abduction (gluteus medius, gluteus minimus, tensor fasciae latae). Think: stepping sideways, keeping your pelvis level when walking.
Sensory: None. Pure motor nerve.
Injury clue: Positive Trendelenburg sign (pelvis drops on the opposite side when standing on one leg). MOTOR ONLY
Inferior Gluteal Nerve
L5 · S1 · S2
Motor: Hip extension (gluteus maximus). Think: climbing stairs, standing up from a chair, or sprinting.
Sensory: None. Pure motor nerve.
Injury clue: Difficulty rising from seated position. Gluteus maximus is the largest muscle in the body: one nerve, one muscle. MOTOR ONLY
Board shortcut: Same roots (L2-L4) feed both the femoral and obturator nerves. Femoral = anterior compartment (flexion + extension). Obturator = medial compartment (adduction). The roots split at the psoas border.
Clinical Images
Tap any image to expand. Visual anchors for the lumbosacral plexus and lower extremity anatomy.
Lumbar plexus branches
Sacral plexus contrast
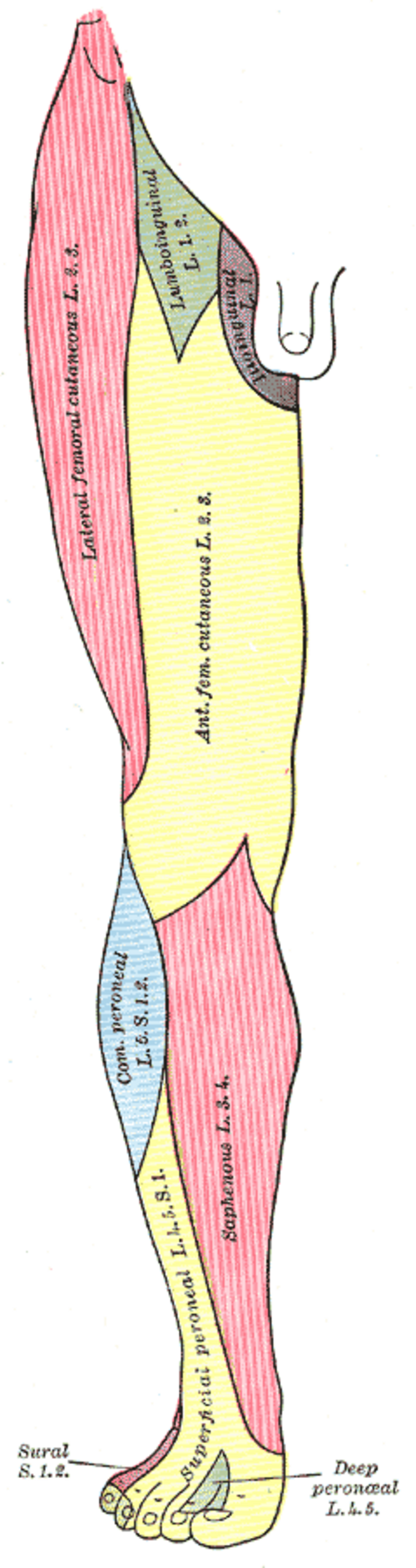
Lower limb sensory map
The Nerve Villains
Each nerve has a signature crime. Tap a card to see what damage it causes when injured.
TAP TO FLIP • tap again to flip back
⚡
Femoral Nerve
L2-L4
tap to see injury pattern
Femoral Nerve Injury
Motor loss: Hip flexion weak (iliopsoas) + knee extension loss (quads). Can't kick, can't climb stairs.
Common cause: Posterior hip dislocation (most common), piriformis syndrome.
👀
Saphenous Nerve
Femoral terminal branch
tap to see injury pattern
Saphenous Nerve Injury
Motor loss: None. Pure sensory branch.
Sensory loss: Medial leg + medial foot. The only femoral branch that crosses the knee.
Reflex: None affected.
Clinical clue: Isolated medial leg/foot numbness with no motor deficit. Often mistaken for diabetic peripheral neuropathy (check distribution carefully).
Common cause: Knee surgery, varicose vein stripping, diabetes.
Nerve Injury Decision Tree
Use this flowchart to work through any lower extremity nerve injury question. Answer each question to find the nerve.
→ Step 1: What is the primary movement that is LOST?
Hip flexion (can't lift the thigh or bend at the hip)
Hip extension (can't push up from a chair or climb stairs)
Hip abduction (can't step sideways; pelvis drops when standing)
Hip adduction (can't squeeze knees together)
Knee flexion + everything below the knee (foot drop, toe weakness)
Femoral nerve (L2-L4). Iliopsoas is the primary hip flexor, powered by the femoral nerve. If there is also knee extension loss, the lesion is proximal to the iliopsoas branch. If knee extension is also lost but hip flexion is spared, the lesion is distal to the iliopsoas branch (after that branch exits). Check the saphenous distribution for medial leg sensory loss (that's the femoral terminal branch). In MS: UMN lesion causes spastic hip flexion (too much tone), not weakness. A nerve block targets the femoral nerve to reduce spastic hip flexors.
Inferior gluteal nerve (L5-S2). Goes to one muscle: gluteus maximus. This is the prime hip extensor. Trendelenburg will be negative because the superior gluteal (abduction) is intact. If the patient also has knee flexion weakness and foot problems, suspect sciatic nerve instead (which also gives hamstrings via posterior thigh). The key: isolated hip extension loss with normal abduction and no below-knee findings = inferior gluteal.
Superior gluteal nerve (L4-S1). Positive Trendelenburg sign: pelvis drops CONTRALATERAL to the lesion when the patient stands on the affected leg. The superior gluteal innervates gluteus medius, gluteus minimus, and tensor fasciae latae. Pure motor nerve. Injury from improper IM injection (use the ventrogluteal or upper-outer quadrant of the gluteus) or hip arthroplasty.
Obturator nerve (L2-L4). Hip adductors (adductor longus, brevis, magnus) are the obturator's domain. A small sensory patch on the medial thigh may also be affected. Pelvic surgery and obturator hernia are the classic mechanisms. Note: the obturator and femoral share roots (L2-L4) but exit the pelvis in different directions. Same neighborhood, different highways.
Sciatic nerve (L4-S3). The largest nerve in the body. Injury causes widespread deficit: hamstrings (knee flexion), everything below the knee via its tibial and common peroneal branches. Look for absent Achilles reflex, foot drop, sensory loss over posterior thigh and below knee. After posterior hip dislocation, suspect sciatic first. If only foot drop with no hamstring weakness, the lesion may be at the common peroneal branch (wraps around fibular head).
→ Step 2: Trendelenburg sign question. The patient stands on the RIGHT leg. The LEFT pelvis drops. Which nerve is injured?
Right superior gluteal nerve
Left superior gluteal nerve
Correct. Right superior gluteal nerve. When you stand on the RIGHT leg, the RIGHT abductors must contract to hold the LEFT pelvis up. If the RIGHT superior gluteal nerve is damaged, the right abductors are weak, the left pelvis drops. The injury is always on the STANDING leg side. Think of it as: the standing leg is the crane, the abductors are the crane arm, and the pelvis is the load. If the crane arm on the standing side is broken, the load (opposite pelvis) drops.
Classic Trendelenburg trap. It's the RIGHT, not the left. When standing on the RIGHT leg, the RIGHT abductors keep the LEFT pelvis up. If the right superior gluteal were intact, the left pelvis stays level. The left superior gluteal would only matter when standing on the LEFT leg. Remember: pelvis drops OPPOSITE to the standing side = nerve injured on the STANDING side.
→ Step 3: A patient has a posterior hip dislocation. What is the first nerve to consider?
Sciatic nerve (exits posterior via greater sciatic foramen)
Femoral nerve (exits anterior under inguinal ligament)
Sciatic nerve is the primary concern. In posterior hip dislocation, the femoral head moves POSTERIORLY and can stretch the sciatic nerve, which exits via the greater sciatic foramen. Check hamstring strength, look for foot drop, test the Achilles reflex, check posterior thigh sensation. However: if only hip extension is lost with no below-knee findings, the inferior gluteal nerve (not sciatic) may be the isolated injury.
Femoral nerve is generally protected in posterior dislocation. The femoral nerve is anterior, passing under the inguinal ligament. A posterior dislocation pushes the femoral head backward, away from anterior structures. Femoral nerve injury is more associated with anterior hip dislocations or groin/inguinal procedures. For posterior dislocations, think sciatic (or inferior gluteal if isolated).
Nerve Elimination
Your patient has spastic hip flexion from an MS plaque. Four clues, four nerves eliminated. Which one remains?
Ready?
Tap "Next Clue" to begin the elimination. Each clue removes one nerve that cannot be causing spastic hip flexion.
Sciatic
Hip extension + knee flexion
Superior Gluteal
Hip abduction
Inferior Gluteal
Hip extension
Obturator
Hip adduction
Femoral
Hip flexion + knee extension
Test Yourself
10 original questions, 5 served at random. Every explanation teaches, not just scores.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.