One neurotransmitter. Four circuits. Four completely different consequences when you block it.
Opening Case
28-year-old woman with schizophrenia has been on risperidone for 6 weeks. She comes in with galactorrhea, amenorrhea, and decreased libido. Her positive symptoms (hallucinations, delusions) are well controlled.
Which dopamine pathway was blocked intentionally? Which one is the collateral damage?
scroll to begin
Overview
The 4 Dopamine Pathways
One neurotransmitter. Four circuits. Blocking one pathway to treat schizophrenia breaks three others.
🧠
Mesolimbic: VTA → limbic (nucleus accumbens). Reward and motivation. Overactive in schizophrenia. Antipsychotics block this pathway to reduce hallucinations and delusions.
🧠
Mesocortical: VTA → prefrontal cortex. Negative symptoms and cognition. Blocking this worsens flat affect, alogia, avolition (the "side effect" of antipsychotics).
●
Nigrostriatal: Substantia nigra → striatum. Movement coordination. Block this → EPS (dystonia, akathisia, bradykinesia, tardive dyskinesia).
The Board Rule: Antipsychotics block all 4 pathways. You want mesolimbic blocked. The other three are collateral damage: EPS (nigrostriatal), hyperprolactinemia (tuberoinfundibular), worsened negative symptoms (mesocortical).
The Pattern
4 Pathways + 1 Danger Zone
Click any pathway on the map or the grid below to see the route, the function, and what breaks when you block it.
1
Mesolimbic
Reward · Urges
2
Nigrostriatal
Movement
3
Tuberoinfundibular
Prolactin Brake
4
Mesocortical
Decisions · Drive
+
CTZ
Antiemetic Target
🤍
Mesolimbic Pathway
VTA → Nucleus Accumbens
The reward and urge circuit. Dopamine floods the nucleus accumbens when you eat, use drugs, or anticipate something pleasurable. This is the "I want it" signal.
In schizophrenia this pathway is hyperactive → generates positive symptoms: hallucinations, delusions, disorganized thought. The brain is producing reward-circuit noise that feels like external voices.
Normal Function
Reward salience, motivation, reinforcement learning. Why heroin feels good and gambling is addictive. Every drug of abuse eventually floods this circuit.
Disease State
Overactive: positive symptoms of schizophrenia. Hallucinations, delusions, paranoia, thought disorganization.
Block it (Antipsychotic)
WANTED D2 block suppresses positive symptoms. This is the therapeutic target. The entire reason antipsychotics exist.
Key Drugs
All antipsychotics (haloperidol, risperidone, olanzapine, quetiapine, aripiprazole). This is the one you WANT to block.
🧠
Nigrostriatal Pathway
Substantia Nigra pars compacta → Dorsal Striatum (Caudate + Putamen)
The movement pathway. Dopamine from the SNpc keeps the basal ganglia in check, enabling smooth coordinated motor output. Lose the dopamine → lose the "go" signal for movement.
This is where Parkinson's disease lives: SNpc neurons die, dopamine disappears, the striatum's inhibitory output goes unchecked, and movement freezes.
Normal Function
Fine motor control, movement initiation, motor learning. Balances direct pathway (go) vs indirect pathway (stop).
Acute dystonia: hours to days. Akathisia: days to weeks. Drug-induced parkinsonism: weeks to months. Tardive dyskinesia: months to years.
⚠️
Board Trap: EPS Timing
The later the EPS, the harder to reverse. Tardive dyskinesia can be irreversible after chronic D2 block causes receptor upregulation. Valbenazine (VMAT2 inhibitor) is FDA-approved for TD.
The prolactin brake. Dopamine tonically inhibits prolactin release from pituitary lactotrophs. This is the one pathway where dopamine's job is purely suppressive.
Block this pathway → brake removed → prolactin floods the system → hyperprolactinemia. This is exactly what happened in our opening case.
Normal Function
Dopamine = prolactin inhibitory factor (PIF). Keeps prolactin at baseline. Without dopamine, prolactin rises automatically.
Block it → Effects
UNWANTED Galactorrhea, amenorrhea, gynecomastia, decreased libido, sexual dysfunction, infertility.
Dopamine and prolactin are inversely linked. During normal pregnancy estrogen suppresses dopamine → prolactin rises → lactation. Drugs that block dopamine mimic this state.
🧠
Mesocortical Pathway
VTA → Prefrontal Cortex
The executive control pathway. Dopamine in the PFC enables working memory, decision-making, goal-directed behavior, and abstract thought.
In schizophrenia this pathway is underactive, generating negative symptoms: flat affect, avolition, alogia, anhedonia, cognitive blunting. These are the hardest symptoms to treat.
Normal Function
Working memory, attention, planning, impulse control, abstract reasoning. Low dopamine here resembles ADHD-like cognitive deficits.
Disease State
Underactive: negative symptoms of schizophrenia. Flat affect, avolition, alogia, anhedonia.
Typical Antipsychotics
WORSENS Blocking D2 here makes negatives worse. Flat affect gets flatter. Already underactive → even more underactive.
Why atypicals are preferred: 5-HT2A block on raphe serotonergic neurons acts as a "release valve" for dopamine in the PFC. More dopamine in cortex → better negative symptom coverage.
🦭
Chemoreceptor Trigger Zone (CTZ)
Area Postrema → Vomiting Center (outside the BBB)
The CTZ is outside the blood-brain barrier , physically in the brain but exposed to blood and CSF. D2 receptors here sample both for toxins, opioids, and dopamine → trigger the vomiting center.
Block D2 here → antiemetic effect. Metoclopramide, haloperidol (low dose), and prochlorperazine all work this way.
Why Outside BBB
Allows the brain to sample blood for toxins and trigger emesis before absorption. The BBB would block this protective signal.
Prochlorperazine, domperidone (stays peripheral, less EPS), haloperidol low dose. All D2 antagonists at the CTZ.
⚠️
Metoclopramide + Tardive Dyskinesia
FDA black box: prolonged use (>12 weeks) risks tardive dyskinesia via nigrostriatal block. TD can be irreversible. Lowest dose, shortest duration. Particularly dangerous in elderly patients.
Quick Recall
Tap Each Pathway
One tap. Front: the name. Back: the punchline. Run through these any time you need a refresh.
1
Nigrostriatal
tap to flip →
Movement Pathway
Substantia nigra → striatum. Movement. Blocked by antipsychotics = EPS. Lost in Parkinson's.
The pathways on a brain. The lesion in Parkinson's. The drug that blocks them. Tap to expand.
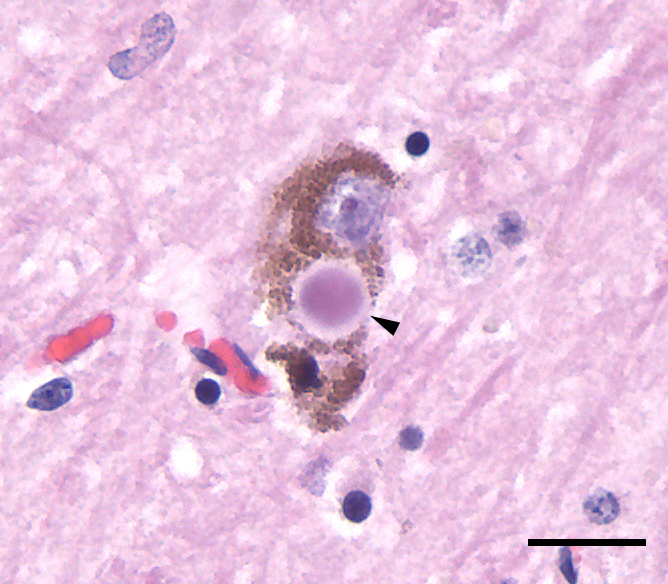
🔬 Lewy Body in SN · tap to expand
Lock It In
Memory Hooks
Three hooks. One for the names, one for the side effect map, one for typical vs atypical.
🔐 Hook 1 · The 4 Names
NMTL = Never Mind The Lost.Nigrostriatal, Mesolimbic, Tuberoinfundibular, LimbicoMesocortical. Four pathways, one phrase.
🔐 Hook 2 · The Side Effect Map
Antipsychotics block D2: good for mesolimbic (psychosis), bad for nigrostriatal (EPS), bad for tuberoinfundibular (prolactin), mixed for mesocortical (negative sx).
🔐 Hook 3 · Typical vs Atypical
First-gen antipsychotics = more D2 block = more EPS plus prolactin. Second-gen = less. The trade-off in one line.
Source
Dopamine Production Sites
Two midbrain nuclei make all the dopamine in the brain. Which one feeds which pathway is the whole game.
SNpc
Substantia Nigra pars compacta
Feeds: Nigrostriatal pathway (motor)
Pigmented neurons (neuromelanin = the "black"). Lose them in Parkinson's and the striatum loses its dopamine drive. The Lewy body you saw earlier lives here.
One nucleus, three projections. Mesolimbic for reward and positive psychosis symptoms, mesocortical for executive function and negative symptoms, tuberoinfundibular for the prolactin brake. The VTA is doing most of the work.
"Dope black smoke needs to Vent." Substantia nigra = black (pigmented). Ventral tegmental = Vent. Two sources, locked into the names.
🧠
Both nuclei sit in the midbrain. SNpc is more lateral, VTA more medial. When a brainstem stroke wipes out the midbrain, both dopamine systems crash together (rare, but a board hook for midbrain anatomy).
Process
5 Dopamine Processes · DOPe to B MVP T
Five places dopamine actually does work. Tap each letter to expand the process and what happens when a D2 antagonist hits it.
Dopamine into the basal ganglia keeps the motor "go" signal alive. Lose it and movement freezes (Parkinson's). Block it and you generate EPS: acute dystonia, akathisia, drug-induced parkinsonism, tardive dyskinesia.
Clinical: Parkinson's = nigrostriatal neurons die. Antipsychotic EPS = same pathway, blocked by drug instead of killed by disease. Same circuit, two ways to break it.
The "I want it" signal. Floods the nucleus accumbens when you eat, get a reward, or take a drug of abuse. Overactive in schizophrenia = positive symptoms: hallucinations, delusions, paranoia.
Clinical: Every drug of abuse converges here. Antipsychotics block this pathway on purpose: D2 antagonism in the mesolimbic line quiets positive symptoms. This is the only block you actually want.
The chemoreceptor trigger zone sits just outside the blood-brain barrier in the area postrema. D2 receptors here sample blood and CSF for toxins. Hit them and you puke.
Clinical: D2 antagonists like metoclopramide, prochlorperazine, and low-dose haloperidol shut the CTZ off and stop nausea. That is why a "psych" drug is a first-line antiemetic.
Too much dopamine in the mesolimbic line = positive psychotic symptoms. Hallucinations (especially auditory), delusions, paranoia, disorganized thought. The "voices" are reward-circuit noise that gets routed as external speech.
Clinical: D2 antagonist antipsychotics treat positive symptoms by damping this circuit. Negative symptoms (flat affect, avolition) come from mesocortical underactivity, which is why typicals can make them worse.
Dopamine tonically inhibits prolactin release from pituitary lactotrophs. Dopamine IS prolactin inhibitory factor (PIF). Remove the brake and prolactin floods the system.
"It is DOPe to B MVP T."Basal ganglia, Mesolimbic, Vomiting center, Psychosis, Tuberoinfundibular. Five places dopamine works. Block any of them and you get a board question.
Wider Map
Neurotransmitter Overview
Where each major neurotransmitter is made, and which disease pops up when it runs too high or too low. Dopamine in context.
N. of MeynertACh source · basal forebrain
Substantia NigraDA · nigrostriatal source
VTADA · meso pathways + TI
Locus CoeruleusNorepinephrine source
Raphe NucleiSerotonin source
NT
Source
HIGH disease
LOW disease
Acetylcholine
"Ace the test like MyNerd"
N. basalis of Meynert · NMJ
Parkinson disease
Alzheimer disease
Dopamine
"Dope black smoke needs to Vent"
SNpc + VTA
Schizophrenia, Huntington
Depression, Parkinson, RLS
Norepinephrine
"No 4 Loco"
Locus coeruleus (pigmented neurons)
Anxiety
Depression
Serotonin
"Sir Raphe"
Raphe nucleus
Serotonin syndrome
Depression, Parkinson
GABA
"Grab aCucumber"
Nucleus accumbens
·
Anxiety, Huntington
⚠
Flagged rows are the board hooks. Alzheimer = LOW ACh from Meynert. Schizophrenia = HIGH dopamine (mesolimbic). Parkinson = LOW dopamine (nigrostriatal). Serotonin syndrome = TOO MUCH 5-HT. Huntington = LOW GABA in the striatum. Memorize the flagged cell, the rest follows.
Circuit Map
Every D2 Blocker Hits All 4 Pathways
The drug doesn't know which pathway you're targeting. Collateral damage is unavoidable.
Haloperidol (typical)
Mesolimbic: treats +sxNigrostriatal: high EPSTI: hyperprolactinemiaMesocortical: worsens -sx
High EPS risk. IV form for acute agitation. Low-dose antiemetic (CTZ only at low doses).
Risperidone (atypical)
Mesolimbic: treats +sxNigrostriatal: moderate EPSTI: WORST prolactinMesocortical: some 5-HT2A
Worst offender for hyperprolactinemia. Also blocks H1 (sedation) and a1 (orthostasis). Our opening case drug.
D2 partial agonist: acts as antagonist in high-dopamine areas, weak agonist in low-dopamine areas. Can cause akathisia. Reverses antipsychotic-induced hyperprolactinemia.
Clozapine
Mesolimbic: treats +sxNigrostriatal: lowest EPSTI: low prolactinMesocortical: best -sx
Gold standard for treatment-resistant schizophrenia. Agranulocytosis risk requires weekly CBC. Best overall efficacy.
The Game
Pathway Elimination Challenge
A patient has a side effect. Eliminate the pathways that did NOT cause it. Find the culprit.
🎯 Reason It Out: Antipsychotic + Gynecomastia
Patient on an antipsychotic develops gynecomastia. Walk the logic, one step at a time.
Step 1. Which pathway does dopamine use to control prolactin release from the pituitary?
Mesolimbic
Nigrostriatal
Mesocortical
Tuberoinfundibular
Yes. Tuberoinfundibular runs hypothalamus to anterior pituitary. It is the dopamine line that controls lactotrophs.
Mesolimbic is reward and positive psychosis symptoms, not pituitary control. Try again.
Nigrostriatal is movement. Block it and you get EPS, not prolactin changes.
Mesocortical is cognition and negative symptoms, not endocrine control. Try again.
↓
Step 2. What does dopamine normally do to prolactin in this pathway?
Stimulates release
Inhibits release
No effect
Right. Dopamine is prolactin inhibitory factor (PIF). Tonic inhibition keeps prolactin at baseline.
Opposite. Dopamine puts the brakes on prolactin, it does not push it.
Dopamine is not neutral here. It is the dominant brake.
↓
Step 3. The antipsychotic blocks D2 in this pathway. What happens to prolactin?
Falls
Rises
Unchanged
Correct. Brake removed = prolactin floods the system = hyperprolactinemia.
If dopamine is the brake and you remove the brake, prolactin cannot fall.
Removing tonic inhibition always shifts the level. It does not stay flat.
↓
Step 4. High prolactin in a male patient causes which clinical findings?
Polyuria + polydipsia
Hypertension + flushing
Galactorrhea + gynecomastia + low libido
Weight loss + tremor
Right. Prolactin drives breast tissue, suppresses GnRH, and tanks libido in both sexes.
That is diabetes insipidus or diabetes mellitus territory, not prolactin.
Carcinoid or pheochromocytoma flavor, not prolactinemia.
That sounds hyperthyroid. Prolactin slows things down, not speeds them up.
Full chain: Antipsychotic blocks D2 in tuberoinfundibular → dopamine normally inhibits prolactin → block dopamine = prolactin rises → galactorrhea + gynecomastia + low libido. Risperidone is the worst offender. Switch to or add aripiprazole (D2 partial agonist) to reverse it.
🎮 Which Pathway?
A patient on haloperidol develops involuntary lip-smacking and tongue movements after 8 months. Which pathway caused this? Eliminate the wrong ones.
Mesolimbic
Reward / urges
Mesocortical
Executive function
Tuberoinfundibular
Prolactin
Nigrostriatal
Movement
Loading clue...
The Exam
Clinical Questions
Cover the answers. Commit. Then click.
Question 1 of 11
A 22-year-old man is brought to the emergency department two days after starting haloperidol for first-episode psychosis because his neck suddenly twists to the left and he cannot relax it. Physical examination reveals painful torticollis with no fever, no confusion, and no lead-pipe rigidity. Laboratory studies show CK 112 U/L (30 to 200), sodium 140 mEq/L (135 to 145), and glucose 91 mg/dL (70 to 99). Which dopamine pathway is responsible?
B is correct. Neck twisting within days of starting an antipsychotic = acute dystonia. This is an extrapyramidal symptom from nigrostriatal D2 blockade. The nigrostriatal pathway runs SNpc to dorsal striatum. Block it acutely → indirect pathway becomes unopposed → muscle groups lock. Treat with diphenhydramine or benztropine IV.
A (Mesocortical): You know how mesocortical is about executive function? Blocking that gives worsened negative symptoms (flat affect, avolition), not motor crises. Mesocortical = cognitive. Nigrostriatal = motor.
C (Tuberoinfundibular): Good instinct on side effects, but TI block gives hormonal effects: galactorrhea, amenorrhea. Not motor rigidity. TI = prolactin. Nigrostriatal = movement.
D (Mesolimbic): That's the therapeutic target, blocking it treats the psychosis. Wanted effect. No motor side effects from mesolimbic block. Think of the four pathways as four circuits in a building: nigrostriatal is the motor circuit. Tripping any other breaker does not flash the motor lights. Only tripping the nigrostriatal breaker causes the motor side effect panel to light up. Break it down: Motor EPS (dystonia, akathisia, parkinsonism, tardive dyskinesia) = nigrostriatal pathway only; mesocortical = cognitive/negative sx; mesolimbic = positive sx treatment target; tuberoinfundibular = prolactin.
Break it down: Motor side effects (EPS) = Nigrostriatal. Every time. Acute dystonia, akathisia, parkinsonism, tardive dyskinesia, all nigrostriatal.
Question 2 of 11
A 45-year-old woman comes to clinic after taking metoclopramide for diabetic gastroparesis for 14 months. Her spouse reports repetitive lip-smacking and tongue thrusting that continue after she holds the medication for one week. Physical examination reveals choreiform orofacial movements without rigidity, fever, or tremor. Laboratory studies show CK 74 U/L (30 to 200), TSH 1.8 uIU/mL (0.4 to 4.0), and sodium 139 mEq/L (135 to 145). What is the most likely diagnosis and mechanism?
A is correct. 14 months = chronic = tardive dyskinesia. Mechanism: chronic D2 blockade in the nigrostriatal pathway causes receptor upregulation (supersensitivity). When hypersensitive receptors get even trace dopamine stimulation → uncontrolled choreiform movements, especially orofacial. Often irreversible. Metoclopramide black box warning.
B (Drug-induced parkinsonism): You know how parkinsonism presents with SLOWNESS and rigidity? This patient has INVOLUNTARY MOVEMENTS, the opposite direction. DIP = dopamine deficiency (receptor blocked acutely). TD = receptor supersensitivity (receptor upregulated chronically). Timing: DIP = weeks. TD = months to years.
D (Acute dystonia): Dystonia happens in hours to days, not 14 months. And dystonia is sustained muscle contraction/twisting, not repetitive lip-smacking. Time course is diagnostic. Think of a calendar as the diagnostic tool: hours to days = dystonia, weeks = parkinsonism, months to years = tardive dyskinesia. The clock hands tell you which drawer to open. Break it down: tardive dyskinesia = months to years of D2 block, orofacial involuntary movements, persists after stopping the drug, receptor upregulation mechanism; acute dystonia = hours to days; DIP = weeks; time course distinguishes all three.
Break it down: Tardive dyskinesia = long duration + orofacial involuntary movements + persists after drug stopped = receptor upregulation from chronic nigrostriatal block.
Question 3 of 11
A patient with schizophrenia treated with typicals shows good control of hallucinations but worsening flat affect, social withdrawal, and inability to initiate activities. This worsening of negative symptoms is most likely due to blockade of which pathway?
C is correct. Mesocortical pathway (VTA → PFC) is already underactive in schizophrenia. Typical antipsychotics block D2 here too → make it even more underactive → worsen flat affect, avolition, alogia. Atypicals are preferred partly because 5-HT2A antagonism increases mesocortical dopamine.
A (Nigrostriatal): Nigrostriatal block causes motor EPS. Not cognitive blunting. The patient would have rigidity or dyskinesia, not worsened affect. Nigrostriatal = motor. Mesocortical = cognitive.
D (Mesolimbic): Mesolimbic block is the GOAL, treating positive symptoms. The positive symptoms are improving here. The negative symptom worsening is a separate pathway. Positive sx = mesolimbic. Negative sx = mesocortical. Good instinct on mesolimbic: you see dopamine blockade and symptom change. The key is WHICH symptoms changed. Positive symptoms improved (mesolimbic working), negative symptoms worsened (mesocortical collateral damage). Think of two dimmer switches: turning down the mesolimbic dimmer is the goal, but typicals also accidentally dim the mesocortical switch and darken the cognitive room. Break it down: typicals block D2 everywhere including mesocortical, which is already underactive in schizophrenia; blocking it further worsens negative symptoms (flat affect, avolition, alogia); atypicals have 5-HT2A antagonism that counteracts this in the PFC.
Break it down: Typicals worsen negative symptoms by blocking the already-underactive mesocortical pathway. This is why atypicals (5-HT2A benefit in PFC) are first-line.
Question 4 of 11
A 30-year-old woman on risperidone reports milky nipple discharge and has not had a period in 3 months. Serum prolactin is 120 ng/mL (normal <20). The physician wants to switch her to an antipsychotic with the lowest risk of continuing this. Which is best?
C is correct. Aripiprazole is a D2 partial agonist. In the tuberoinfundibular pathway, it provides enough dopamine signal to maintain prolactin suppression. It can actually LOWER prolactin and is used specifically to treat antipsychotic-induced hyperprolactinemia. Risperidone is worst; aripiprazole is the fix.
A (Haloperidol): Good instinct: haloperidol causes less prolactin elevation than risperidone. But it is still a pure D2 antagonist that blocks the tuberoinfundibular pathway and maintains hyperprolactinemia. You need a partial agonist, not just a less-guilty full blocker.
B and E (Fluphenazine): Both are typical antipsychotics, pure D2 antagonists with potent nigrostriatal block. Moving from risperidone to fluphenazine would not fix the prolactin and would add EPS risk. Think of trying to fix a faucet dripping too fast by replacing it with an equally broken faucet: the problem is the mechanism (full D2 block), not the brand. You need a different mechanism entirely (partial agonism). Break it down: antipsychotic-induced hyperprolactinemia = tuberoinfundibular D2 block removes the dopamine brake on prolactin; fix = partial agonist (aripiprazole) provides enough D2 signal to suppress prolactin; pure D2 antagonists cannot fix this regardless of potency.
Break it down: Antipsychotic-induced hyperprolactinemia: switch to or add aripiprazole (D2 partial agonist). It reverses the prolactin elevation via partial agonism at tuberoinfundibular D2 receptors.
Question 5 of 11
A 56-year-old woman is evaluated on the oncology service for nausea after chemotherapy. One episode is treated with ondansetron, and a later episode at an outside urgent care is treated with haloperidol. Physical examination after haloperidol reveals jaw stiffness and hand tremor; after ondansetron she had no abnormal movements. Laboratory studies show sodium 138 mEq/L (135 to 145), calcium 9.4 mg/dL (8.5 to 10.5), and CK 96 U/L (30 to 200). Which principle best explains why one antiemetic causes extrapyramidal symptoms and the other does not?
D is correct. Pure receptor biology. Haloperidol blocks D2 everywhere including the nigrostriatal pathway → EPS. Ondansetron blocks 5-HT3 receptors (serotonin, not dopamine). The CTZ has both D2 and 5-HT3 receptors. Ondansetron hits 5-HT3 only → no nigrostriatal D2 block → no EPS. Completely different receptor, completely different side effect profile.
E (Dose-dependent): Good instinct: lower haloperidol doses do have less EPS. But ondansetron has ZERO EPS because it has zero D2 affinity. A receptor it does not bind cannot cause EPS. The problem is the receptor target, not the dose.
B (BBB): Both drugs act at the CTZ (outside BBB). But haloperidol also penetrates INSIDE the BBB to the nigrostriatal pathway. Ondansetron does not cause EPS regardless of BBB permeability because it has no D2 affinity at all. Think of a lock with two key types: ondansetron is a 5-HT3 key that only fits one lock. No matter where it travels, it cannot open the D2 lock that triggers EPS. Haloperidol is a D2 master key that opens the nigrostriatal lock wherever it reaches. Break it down: ondansetron = 5-HT3 antagonist, zero D2 affinity, zero EPS possible; haloperidol = D2 antagonist, blocks nigrostriatal wherever it penetrates; receptor affinity determines EPS risk, not BBB permeability or dose.
Break it down: Ondansetron: 5-HT3 only, zero dopamine block, zero EPS. Haloperidol: D2 block everywhere including nigrostriatal, EPS. Different receptors = different consequences.
Question 6 of 11
A 68-year-old man with a long history of Parkinson's disease develops new-onset visual hallucinations and paranoia after his levodopa dose was increased. His tremor and rigidity are well controlled. Which antipsychotic is the safest first-line choice?
D is correct. Parkinson's already has a wrecked nigrostriatal pathway. Any drug that blocks D2 there will make movement worse. Quetiapine has the lowest D2 affinity of the atypicals and the lowest EPS risk, so it can damp the hallucinations without crashing the motor system. Pimavanserin (5-HT2A inverse agonist, no D2 block) is also FDA-approved for Parkinson's psychosis and is even safer when available.
A and E (Haloperidol, Fluphenazine): Both are high-potency typicals. Strong nigrostriatal D2 block on top of an already dopamine-depleted SNpc: the patient ends up frozen. Avoid in any Parkinson's patient.
B (Risperidone): More D2 affinity than quetiapine, plus the worst hyperprolactinemia of the atypicals. Will worsen Parkinson's motor symptoms.
C (Olanzapine): Lower EPS than risperidone but still meaningful D2 block. Quetiapine wins on the motor-safety axis. Good instinct on olanzapine: it is lower-EPS than risperidone and sounds like a reasonable compromise. But in Parkinson's, even moderate D2 block at an already depleted nigrostriatal pathway can cause significant motor deterioration. Think of adding friction to a car engine that is already running on fumes: even a small additional drag can stall it. Quetiapine's minimal D2 affinity is the least additional friction available. Break it down: Parkinson's psychosis treatment = quetiapine (lowest nigrostriatal D2 affinity among atypicals) or pimavanserin (5-HT2A inverse agonist, zero D2 block); avoid all typicals and most atypicals; less D2 block = less motor harm to an already depleted system.
Break it down: Parkinson's psychosis: quetiapine or pimavanserin. Avoid every typical and most atypicals. Less D2 block = less motor harm.
Question 7 of 11
A 19-year-old man with first-episode psychosis is started on haloperidol. Six hours later he is writhing in his seat, unable to sit still, repeatedly standing up and pacing. He says he feels intensely restless. Which best describes the cause and treatment?
C is correct. Subjective restlessness plus the motor inability to sit still, hours to weeks after starting a high-potency D2 blocker, equals akathisia. Mechanism: nigrostriatal D2 block disrupts the basal ganglia balance. Treatment: lower the dose if possible, plus propranolol (beta blocker), benzodiazepines, or anticholinergics like benztropine.
A (Worsening psychosis): A worsening patient does not describe the feeling as restlessness with a need to move. Increasing the dose makes akathisia much worse, fast. Wrong direction.
B (Acute dystonia): Dystonia is sustained muscle contraction (oculogyric crisis, torticollis, laryngospasm), not pacing. Diphenhydramine is right for dystonia, wrong for akathisia.
D (Tardive dyskinesia): TD takes months to years and shows involuntary orofacial movements. Six hours rules it out.
E (NMS): NMS shows fever, autonomic instability, lead-pipe rigidity, altered mental status, and elevated CK. Pacing without those features is not NMS. Good instinct on NMS: it is a dangerous antipsychotic complication and the urge to not miss it is valid. NMS requires the full constellation: fever + rigidity + autonomic instability + AMS + elevated CK. Restless pacing with subjective inner restlessness and none of those features is akathisia, not NMS. Think of NMS as a four-alarm fire and akathisia as an anxiety attack: both are uncomfortable, but the smoke detector tells you which is which. Check for fever and rigidity first. Break it down: akathisia = subjective restlessness + inability to sit still + hours to weeks after starting antipsychotic + NO fever/rigidity/AMS; treatment = propranolol or benzodiazepine, lower dose if possible; increasing the dose worsens akathisia.
Break it down: Restlessness + cannot sit still + just started antipsychotic = akathisia. Propranolol or benzo. Do not raise the dose.
Question 8 of 11
A 35-year-old woman comes to neurology clinic because she uses prochlorperazine several times each month for migraine-associated nausea and asks why her clinician keeps limiting refills. She previously took metoclopramide for gastroparesis and remembers the same warning. Physical examination reveals no resting tremor, no rigidity, and no current orofacial movements. Laboratory studies show prolactin 18 ng/mL (less than 20), CK 82 U/L (30 to 200), and glucose 94 mg/dL (70 to 99). Which mechanism best explains why both drugs share this long-term risk?
B is correct. Prochlorperazine (phenothiazine, sold as Compazine) and metoclopramide are both D2 antagonists. Their antiemetic effect comes from blocking D2 at the CTZ, but they also cross into the nigrostriatal pathway. Chronic D2 block there causes receptor upregulation (supersensitivity), and trace dopamine then triggers uncontrolled choreiform movements: tardive dyskinesia. Both drugs carry FDA warnings.
A (5-HT3): That is ondansetron, granisetron, palonosetron. Different receptor, no nigrostriatal D2 effect, no TD risk.
C (Hyperprolactinemia): Good instinct: both drugs do raise prolactin via the tuberoinfundibular pathway. But high prolactin alone does not cause dyskinesia. The motor problem comes from nigrostriatal D2 block, a separate pathway. Prolactin and EPS are parallel consequences of D2 block at two different locations.
D (H1): Diphenhydramine and meclizine are H1 antihistamines. They are not the antiemetics that cause TD. Wrong receptor target entirely.
E (VMAT2): That is tetrabenazine and valbenazine, which actually TREAT TD by depleting striatal dopamine. Opposite mechanism from the offenders. Think of VMAT2 inhibitors as the fire extinguisher for a fire that D2 antagonists started: you would not say they share the same mechanism just because they both involve dopamine. The causal chain runs in opposite directions. Break it down: metoclopramide and prochlorperazine cause TD via chronic nigrostriatal D2 block causing receptor upregulation; 5-HT3 antiemetics (ondansetron) have zero D2 affinity and zero TD risk; VMAT2 inhibitors treat TD by depleting dopamine, opposite direction.
Break it down: Any chronic D2 antagonist that reaches the nigrostriatal pathway can cause TD. Metoclopramide and prochlorperazine are the two big antiemetic offenders.
Question 9 of 11
A 24-year-old man with first-episode psychosis is started on a D2 antagonist. Match the following dopamine-driven process to the patient finding it produces when D2 is blocked at that site: a 38-year-old woman on the same drug class develops new milky breast discharge and a missed period. Which of the five dopamine processes ("DOPe to B MVP T") best explains her finding?
E is correct. Galactorrhea and amenorrhea are the signature of tuberoinfundibular D2 block. Dopamine normally inhibits prolactin release from anterior pituitary lactotrophs. Remove the dopamine brake = prolactin rises = milky discharge plus suppressed GnRH and missed periods. Risperidone is the textbook offender.
A (Basal ganglia): Block here gives EPS: dystonia, akathisia, parkinsonism, tardive dyskinesia. Motor findings, not endocrine. Think of the five letters as five separate switchboards in the brain: flipping the B switchboard lights up the motor panel, not the breast tissue panel.
B (Mesolimbic): This is the therapeutic block, the reason antipsychotics exist. Blocking mesolimbic quiets positive psychosis symptoms. No prolactin link at all.
C (Vomiting center): CTZ D2 block is antiemetic. It does not reach the pituitary stalk. Wrong switchboard, wrong building.
D (Psychosis): P is just the named consequence of mesolimbic overactivity, the same circuit as B in this mnemonic. Choosing P or B here is choosing positive symptoms, not endocrine effects. Think of milk and periods like a kitchen faucet: dopamine is the hand on the valve keeping prolactin off. Block dopamine in the tuberoinfundibular line and the hand lifts; prolactin floods. Only the T switchboard runs that valve. Break it down: galactorrhea plus amenorrhea = tuberoinfundibular D2 block = T in DOPe to B MVP T. The other four processes do not regulate prolactin.
Break it down: Milky discharge + missed period on a D2 antagonist = T (tuberoinfundibular). Aripiprazole (D2 partial agonist) is the fix because it puts the brake back on.
Question 10 of 11
A 72-year-old man is brought in by his daughter for progressive memory loss over 2 years. He repeats himself, cannot recall his daughter's recent visit, and was found wandering at night. Brain MRI shows generalized cortical atrophy with hippocampal involvement. Cholinesterase inhibitor therapy is started. Loss of which neurotransmitter from which anatomic site best explains his disease?
C is correct. Slow memory decline plus hippocampal and cortical atrophy in a 72-year-old equals Alzheimer disease. Alzheimer kills cholinergic projection neurons in the nucleus basalis of Meynert (basal forebrain), so cortex-wide acetylcholine drops. That is exactly why cholinesterase inhibitors (donepezil, rivastigmine, galantamine) help: less ACh degradation = more ACh available at the synapse. "Ace the test like MyNerd."
A (Dopamine from SNpc): That is Parkinson disease: resting tremor, bradykinesia, rigidity, postural instability. SNpc neurons die, nigrostriatal dopamine drops. Movement problem, not a memory-first problem. Wrong nucleus, wrong NT, wrong disease.
B (Serotonin from raphe): Low raphe serotonin shows up in depression, not in a hippocampal-atrophy dementia. SSRIs treat that, not cholinesterase inhibitors.
D (Norepinephrine from LC): Locus coeruleus neurons do die in Alzheimer, but the cholinergic deficit from Meynert is the cell loss that drives the cognitive picture and is what the cholinesterase inhibitor targets. LC loss explains anxiety and arousal changes, not the cholinesterase-inhibitor mechanism.
E (GABA from nucleus accumbens): GABA deficiency in the striatum drives Huntington chorea, not memory loss. Wrong NT, wrong region, wrong disease entirely. Think of each source nucleus as a power plant feeding one part of the city: when the cholinergic plant in the basal forebrain dims, the memory district browns out, and only ACh-boosting drugs help. Boosting dopamine, serotonin, or norepinephrine cannot relight a district they do not feed. Break it down: Alzheimer = low ACh from nucleus basalis of Meynert; Parkinson = low DA from SNpc; depression = low NE (LC) or 5-HT (raphe); Huntington = low GABA from striatum; cholinesterase inhibitors only help when the deficit is ACh.
Break it down: Alzheimer dementia + cholinesterase inhibitor response = low ACh from the nucleus basalis of Meynert. Match the drug to the source nucleus.
Question 11 of 11
A 26-year-old woman on sertraline for major depression is started on tramadol after a wrist fracture. Six hours later she develops tachycardia, hyperthermia (39.4 C), diaphoresis, agitation, clonus in the lower extremities, and hyperreflexia. Excessive activity of which neurotransmitter, originating from which brainstem nucleus, is responsible?
B is correct. SSRI plus tramadol (which itself blocks serotonin reuptake and has weak serotonin agonist activity) within hours = serotonin syndrome. Triad: autonomic instability (fever, tachycardia, sweating) + neuromuscular excitation (clonus, hyperreflexia, rigidity, especially lower extremities) + mental status change (agitation). The source is the raphe nuclei in the midline brainstem, which project serotonin everywhere. Stop the offending drug, supportive care, cyproheptadine if severe. "Sir Raphe."
A (Dopamine from VTA): Hyperdopaminergic states present as psychosis or stimulant intoxication, not as fever plus lower-extremity clonus. Neuroleptic malignant syndrome looks similar but is from D2 blockade (low dopamine), and patient is not on an antipsychotic. Wrong NT and wrong direction.
C (Norepinephrine from LC): A noradrenergic storm (cocaine, pheochromocytoma) gives hypertension and tachycardia but does not produce the classic lower-extremity clonus and hyperreflexia. Drug history points to a serotonergic cause, not adrenergic.
D (Acetylcholine from Meynert): Cholinergic crisis (organophosphates, neostigmine overdose) shows SLUDGE: salivation, lacrimation, urination, defecation, GI cramps, emesis, plus bronchospasm and miosis. Not this picture.
E (GABA from accumbens): Excess GABA causes sedation and respiratory depression (benzo overdose), the opposite of this hyperactive picture. Wrong NT entirely. Think of the raphe as a postal hub in the brainstem sorting serotonin letters to every neighborhood. Tramadol + SSRI is like jamming the return-to-sender mailbox: letters pile up, every neighborhood gets flooded, and the body lights up with fever, twitchy reflexes, and agitation. Only the raphe runs that mail route. Break it down: serotonin syndrome = excess 5-HT from raphe nuclei = autonomic instability + neuromuscular excitation + altered mental status, especially with SSRI + tramadol/MAOI/linezolid/MDMA combos; treat by stopping the offender, supportive care, cyproheptadine if severe.
Break it down: SSRI + tramadol + fever, clonus, hyperreflexia = serotonin syndrome = excess 5-HT from the raphe nuclei. The source nucleus pins the NT, and the NT pins the diagnosis.
🎯 Case Resolution
Back to our 28-year-old on risperidone:
Intentional target: Mesolimbic pathway. D2 block suppressed her positive symptoms (hallucinations, delusions). Working as intended.
Collateral damage: Tuberoinfundibular pathway. D2 block removed the prolactin brake → galactorrhea, amenorrhea, decreased libido. Risperidone is the worst offender because it has particularly high affinity for pituitary D2 receptors.
Management: Switch to or add low-dose aripiprazole. Its partial agonism at tuberoinfundibular D2 receptors normalizes prolactin while maintaining psychosis control.
clinical Walkthrough
clinical Walkthrough
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed June 2026
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.