Understanding protein metabolism, transaminases, and liver damage patterns
When the Body Breaks Down Proteins
After glucose and glycogen stores are depleted, your body turns to proteins as an energy source. This process, called amino acid catabolism, is essential for survival during fasting or metabolic stress.
The Core Process: Transaminases
Breaking down amino acids requires removing the amine group (NH₂). This is where transaminases come in→enzymes that transfer amine groups between molecules:
Transfer OFF: Remove amine groups to break down amino acids
Transfer ON: Add amine groups to synthesize new amino acids for proteins
Key Point: Every Amino Acid Needs Its Own Enzyme
With 20 common amino acids, there are theoretically 20 different transaminases. However, two transaminases (AST, ALT) plus one transferase (GGT) are the three clinically important liver enzymes.
B6 Rule: The true transaminases (AST and ALT) require Vitamin B6 (Pyridoxine) as a cofactor. GGT does NOT require B6 (it is not a transaminase). No B6 = no AST/ALT activity.
The Three Heavy-Hitters
Tap each card to flip. Front shows the enzyme and where it leaks from. Back shows the actual reaction and the clinical move it forces on test day.
GGT
Gamma-Glutamyl Transferase
BILE DUCT MEMBRANES
The booze marker. Sits on hepatocyte and bile duct membranes. Does not need vitamin B6.
When it leaks: alcohol use or anything blocking bile flow lights this up. AST and ALT can stay quiet while GGT climbs.
tap to flip
Reaction & Clinical Move
Transfers a gamma-glutamyl group
Not a true transaminase. Hands gamma-glutamyl groups from glutathione to other peptides at the cell membrane.
Glutathione + AA → gamma-glutamyl-AA + cysteinylglycine
Why it matters: elevated ALP could be liver OR bone. GGT up alongside ALP locks it as liver. GGT alone with normal AST/ALT often means quiet alcohol use.
Move: see GGT up + AST > ALT (2:1 or higher) and the alcohol picture is sealed before you read another lab.
AST
Aspartate Aminotransferase
CYTOPLASM · MITOCHONDRIA
The double agent. Two copies, two compartments. That is exactly why alcohol blows the ratio open.
When it leaks: any liver insult drops the cytoplasmic copy. Add mitochondrial damage (alcohol) and the second copy spills too. Now AST runs ahead of ALT.
tap to flip
Reaction & Clinical Move
Swap an amine for an aspartate
True transaminase. Needs vitamin B6 (pyridoxal phosphate). Drives the malate-aspartate shuttle that ferries NADH into mitochondria.
amino acid + OAA → alpha-keto acid + aspartate
Why it matters: AST also lives in heart, skeletal muscle, and red cells. Bumps from rhabdo, MI, or hemolysis can fake liver disease if you forget to check ALT and CK.
Move: AST > ALT in a heavy drinker = alcoholic hepatitis. AST > ALT with normal ALT and high CK = think muscle, not liver.
ALT
Alanine Aminotransferase
CYTOPLASM ONLY
The liver loyalist. Single copy in the cytoplasm of hepatocytes. No mitochondrial twin to leak.
When it leaks: something dented the hepatocyte cell membrane. ALT up = liver, almost always. The most specific of the three.
tap to flip
Reaction & Clinical Move
Swap an amine for an alanine
True transaminase. Also B6-dependent. Pulls amine groups onto pyruvate to make alanine, which the muscle ships to liver in the alanine cycle.
amino acid + pyruvate → alpha-keto acid + alanine
Why it matters: ALT outlasts AST in viral hepatitis. So a 1:1 ratio with ALT trending higher than AST over a week screams viral, not booze.
Move: AST and ALT both up, ratio near 1:1, ALT staying high longest = viral hepatitis story.
ALT vs AST Memory: ALT = "Alanine Liver Tissue" (cytoplasm only, specific to liver). AST = "Aspartate Spans the Structures" (cytoplasm + mitochondria, less specific).
Liver Enzyme Location Map
Understanding WHERE these enzymes live is critical for interpreting liver damage patterns. When membranes break, different enzymes "leak out." AST and ALT are the true transaminases (require B6). GGT is a transferase in bile duct epithelium and hepatocyte membranes.
Cytoplasm
AST
Cytoplasmic form (one copy)
ALT
ONLY location
Mitochondria
AST
Mitochondrial form (one copy)
GGT
Bile ducts and hepatocyte membranes (NOT a transaminase)
Board Trap: Students memorize that AST and ALT are elevated in liver disease but don't understand the mechanism. The KEY is understanding which membranes are damaged and which enzymes leak out as a result.
Where Do the Carbon Chains Go?
After transaminases strip off amine groups, the carbon skeletons must be catabolized. These amino acid carbons enter the Krebs Cycle at 6 different points:
Pyruvate
Gateway to acetyl-CoA
Acetyl-CoA
Direct entry
α-Ketoglutarate
Krebs cycle intermediate
Succinyl-CoA
Krebs cycle intermediate
Fumarate
Krebs cycle intermediate
OAA
Oxaloacetate
These multiple entry points explain why amino acid metabolism is so flexible→the body can use amino acids for energy, gluconeogenesis, or lipogenesis depending on metabolic needs.
Interactive: Liver Damage Detector
Drag the sliders or load a board scenario. Watch the readout name the damage pattern from which enzymes leaked out. The AST:ALT ratio and the height of the numbers decide everything.
AST Level (U/L)100
ALT Level (U/L)100
GGT Level (U/L)50
DIAGNOSIS
Adjust the sliders
AST:ALT Ratio
1:1
Max Enzyme
100
Liver Damage Patterns: Battle Cards
These are the classic patterns you MUST know for boards. Each represents different mechanisms of cellular damage.
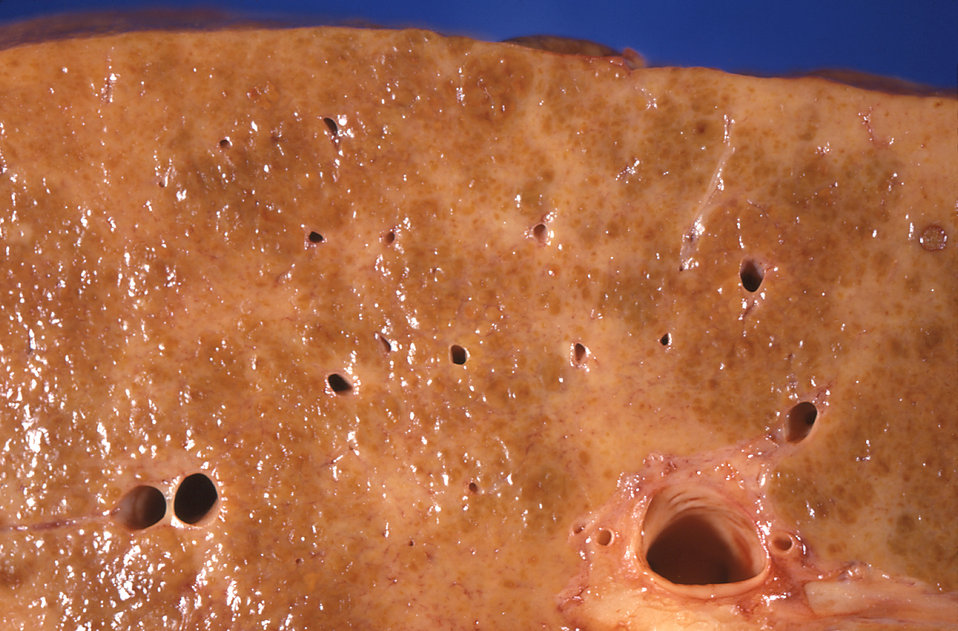
📷 Cirrhotic liver · tap to expand
📷 Fatty liver · tap to expand
📷 Scleral icterus · tap to expand
📷 Alcoholic hepatitis · tap to expand
HEPATITIS
Trace ItInflammation
Membrane HitCell membrane only
What Leaks1 AST (cyto) + 1 ALT
AST:ALT Ratio1:1
GGT LevelNormal/Low
Cause: Viral (A, B, C), autoimmune, or drug-induced
ALCOHOLIC HEPATITIS
Trace ItCell + mitochondrial damage
Membrane HitBoth membranes broken
What Leaks2 ASTs + 1 ALT + GGT
AST:ALT Ratio2:1 or higher
GGT LevelElevated
Signature: AST > ALT (opposite of viral hepatitis)
HEPATIC NECROSIS
Trace ItCell death (cytotoxic)
Membrane HitDESTROYED
What LeaksEVERYTHING massively
Enzyme Levels1000s (AST & ALT)
Common CauseFat-soluble drugs
Hallmark: Massive enzyme elevations (>1000 U/L)
CIRRHOSIS
Trace ItFibrosis/scarring
Enzyme PatternMild elevation or normal
Key Finding↓Albumin, ↑PT
WhyCan't make proteins
Clinical SignPortal hypertension
Trick: Enzymes aren't THAT high but synthetic function is shot
Memory Hook: The Ratio Rule
• AST:ALT = 1:1 → Regular hepatitis (cell membrane problem)
• AST:ALT = 2:1 → Alcoholic hepatitis (cell + mitochondria problem)
• AST:ALT > 5:1 → Think cirrhosis or other causes
• Both in 1000s → Necrosis (hepatocyte death)
The AST:ALT Read: Decision Tree
Real patients hand you a number panel, not a diagnosis. Walk the same fork an attending uses at the bedside. Guess each step before it opens. This is a decision-treechallenge: commit, then reveal.
Step 1 · A panel comes back with both transaminases up. First fork: how high are the numbers?
In the THOUSANDS (both over 1000 U/L)
In the tens-to-hundreds (under ~500 U/L)
Necrosis branch. Numbers in the thousands mean cells are dying, not just inflamed. The short list is acetaminophen toxicity, ischemic hepatitis ("shock liver"), and fulminant acute viral hepatitis. Check INR and pH next, because synthetic failure is the thing that kills. The rule: over 1000 = count the zeros, think cell death.
Inflammation branch. Mild to moderate elevations point at chronic or smoldering injury, not acute death. Now the RATIO does the sorting. The rule: under 500 = let the AST:ALT ratio pick the cause.
Step 2 · Numbers are moderate. Now look at the ratio. AST is more than double the ALT and the GGT is up. What does that combination name?
AST:ALT > 2:1 with high GGT
ALT > AST, GGT normal
Alcohol. The mitochondrial copy of AST only spills when something wrecks mitochondria, and acetaldehyde from alcohol does exactly that. The second AST source flips the ratio past 2:1. GGT sits on the cell membrane and lights up with alcohol use, sealing it. The rule: AST > 2x ALT plus high GGT = alcohol did it.
Viral or non-alcoholic (NAFLD/NASH). When only the cell membrane is hit, cytoplasmic ALT (liver-specific, longer half-life) leads. A roughly 1:1 ratio with ALT on top and a quiet GGT is the viral/fatty-liver picture. The rule: ALT on top with calm GGT = viral or fatty liver, not booze.
Step 3 · New patient: transaminases only mildly up, but ALP is high. Liver or bone? Which single lab settles it?
Check GGT
Check albumin only
GGT is the tiebreaker. Alkaline phosphatase comes from BOTH liver (bile ducts) and bone. GGT lives in the biliary tree and is NOT in bone. High ALP plus high GGT = cholestatic liver source. High ALP with a normal GGT = bone. The rule: GGT up confirms the ALP is from liver, every time.
Albumin tracks synthetic function, not the source of an isolated ALP. A low albumin and high INR tell you the liver cannot DO its job (the cirrhosis story), but they cannot tell you whether a high ALP came from bile ducts or bone. For that one question, GGT is the discriminator. The rule: isolated high ALP needs GGT, not albumin, to localize it.
Bonus: Why Rapid Growth Matters for Metabolism
During periods of rapid growth, amino acid catabolism and the Glycerol-3-Phosphate Shuttle kick into high gear. These periods include:
This is why critically ill patients need high-protein nutrition→their bodies are in a "growth mode" metabolically, even though they're not actually growing!
Board-Style Quiz
Test your knowledge with 10 realistic clinical scenarios. You'll see 5 random questions. Confetti on success!
Board-Style Walkthrough
Board-Style Walkthrough
Original board-style vignettes built around the AST:ALT read. One at a time, shuffled, never-repeat. Right-click (or long-press) to cross out a choice. Double-click (or double-tap) to highlight one. Tools lock once you answer.